In medicine, for the first time, the norms for the time of admission by doctors of patients were approved. When compared with the time norms that were in use earlier, it can be seen that the indicators for medical specialists have increased. Based on this, it can be assumed that the appearance of updated standards will be followed by changes in the structure of clinic doctors and their total number.
New norms for doctor's appointments
Unfortunately, the order of the Ministry of Health of Russia dated 02.06.2015 No 290n, which determined the norms for the time for receiving patients from doctors of certain specialties, sins with the uncertainty of terminology and wording. This may result in discrepancies in some paragraphs of the recently issued order.
Thus, paragraph 1 of the Order of the Ministry of Health No. 290n reports that standard standards and norms for the time of a doctor's appointment can be applied both for medical care in outpatient clinics and when visiting potential patients by a doctor directly at home.
This can also be interpreted as we are talking about specific norms of time for the reception of patients by doctors directly in the clinic or at home, and as average norms for the reception of patients by doctors anywhere.
But meanwhile, the norms of time for the reception of patients by doctors during “home” visits are usually two to three times more than the norms for the time spent on visiting a patient in a clinic. The level of settlement of residents, and the time that has to be spent on moving around the site, and the size of the site, even whether there are elevators in the entrances of patients' houses, etc. play a role here. Because of this, it can hardly be unequivocally stated that these indicators of the required time can be similar to each other.
But the norms of time for patients to receive patients by doctors are the average figures between the time spent on visiting patients in the clinic and coming to the patient at home. And in each case, it will be necessary to separate these norms depending on the differentiation of the types of visits to potential patients at the place where medical care was provided, at the patient's home or in the clinic. Depending on the results, the average time norms determined for visits to patients will change.
The conclusion is that the points of this recently adopted document clearly need to be detailed and clarified. Probably, the order of the Ministry of Health still refers to the norms of time for patients to be seen by doctors directly in the clinic. But then in the order of the Ministry of Health there must be a definition of the required standard amount of time for a “home” visit. In addition, it is necessary to determine how these time standards should operate and how they will be changed if necessary. Clarification also requires the question of the norms for the time of admission of patients by doctors, which takes place purely with a preventive purpose. Moreover, the conditions for the application of these standards are not defined in the order, it says only - 60-70% of the norms of the time used associated with a visit by one patient to a medical specialist in connection with the disease. However, an appointment for each appointment of a potential patient with a doctor is made without regard to the purpose of his visit.
Thus, if a visit to a patient who has not yet become ill for a purely prophylactic purpose takes place during a regular visit to the doctor receiving him, then the standard norms for the admission of patients by doctors cannot be accurately differentiated by the purpose of the visit - whether it was due to the onset of the patient's illness or was carried out with the purpose of preventing the onset of the disease. Based on the foregoing, it is extremely necessary to make a clarification in paragraph 6: “a visit to a doctor for a preventive purpose, performed on specially allotted days or hours of admission.”
! If you want to increase the efficiency of your clinic and increase your income, then rather try from Klinikon. With its help, you automate most of the routine processes, free up more time for your employees and increase the profitability of your business. We are trusted by more than 2500 beauty salons throughout Russia !
Time limits for the appointment of medical specialists - expectation and reality
If we focus on timekeeping data, the standard time spent on processing and analyzing medical documentation, which is predicted by the order, coincides with reality only for pediatricians. For example, for a therapist, the time spent on processing and analyzing patient data and other medical documentation is about 40%, for a family doctor - another 3% more. It turns out to be very problematic to meet the set time limits for the reception of medical specialists.
When distributing the time spent on the preparation and analysis of medical documentation in accordance with the standards in the order, in fact, we are faced with a sharp decrease in the volume of collected statistical information. In the future, this is fraught with a lack of statistics on which important medical research is based.
The order mentions adjustment factors that are more applicable to standards and plans for the number of visits to patients, but not to the average norms for the appointment of medical specialists, taking into account each visit. It is extremely difficult to imagine that medical clinics will change entire industry standards the norms for the reception of medical specialists for some one or two minutes. For edits of this order, it is still advisable to use much more significant numbers.
For example, if you add up all the above corrections, then in total they will amount to only 0.15, that is, only some two or three minutes. Table No1 compares the previously adopted, valid before the introduction of order No290-n, the estimated standards of time for a visit, verified in accordance with the standards for such documents as:
- order of the Ministry of Health of the USSR dated 23.09.1981 N1000 "On measures to improve the organization of the work of outpatient clinics" (Order N1000)
- Order No. 290n of the Ministry of Health of the Russian Federation,
- statistical data received from analysts of the All-Russian Research Institute. N. A. Semashko.
Table 1. Comparative data on the norms of appointment time for specialists for 1 visit, min.
Order No. 1000 in the USSR approved the design workload standards for doctors, according to which it was possible to eventually calculate the time limits for the appointment of specialist doctors. Subsequently, it was believed that these figures had already lost their validity.
Comparative Table 1 presents data on time standards, which were preliminarily calculated to be used as weighted averages in differentiating and highlighting the proportions of participants in the structure of clinic visits. The figures were obtained by counting the number of adult patients and children. The use of these data was regulated by the information letter of the Ministry of Health and Social Development of Russia dated December 22, 2011 No 20–2/10/1–8234. This letter was just to this day the last of all existing documents of this kind, which mentions data on the standards of time standards for doctors.
To what extent are the time limits for receiving patients by doctors increasing?
The time spent on visiting one potential patient with a pediatrician and an ophthalmologist, approved by the new Order No. 290n, is quite close to the data that were obtained as a result of statistics analytics during regulatory research work at the All-Russian Research Institute. N. A. Semashko.
Differences between the old data and the new norms of time for patients to see doctors are less than a minute. However, it should also be noted that the increase in the norms of time for visiting a potential patient for an otorhinolaryngologist, recommended by Order No. 290n, is as much as 20% compared to analytical data, and for a neurologist and gynecologist the difference is almost unrealistic - as much as 40%.
It is worth considering that such global changes clearly require a rethinking of the economic assessment of the situation in medicine. It is still difficult to predict how the application of such new time standards will affect the number and number of positions of medical specialists in clinics.
Calculation of the necessary and sufficient number of posts of outpatient doctors
Calculations of the necessary and sufficient number of outpatient doctors, as a rule, are carried out according to the standard method of labor rationing. The calculation source is the use of indicators of two groups of data: the norms of time for patients to see doctors and the number of standard visits. Let us describe the main stages of calculations.
Formula 1. Planned function of a medical position (F)
F = B x k / t, (1)
where B is the annual budget of the working time of the position of the medical worker;
k - the applied factor for the use of the doctor's working time (RVV) for the main activity;
t is the cost of RVV for a medical and diagnostic visit to a polyclinic, or an appeal in connection with a disease.
The coefficient of use of RVV (k) directly depends on what is included in the components of the temporary norms for the reception of patients by doctors. Experience of rationing labor activity physicians quite clearly shows that an outpatient doctor daily out of 6.5 hours of working time with a 6-day working week spends about half an hour on work not related to diagnostic activities or treating patients. For example, time goes to business calls, necessary meetings or conferences, etc. Therefore, k = 0.923 x (6.5 - 0.5) / 6.5. This correction factor is usually used in all modes of work of health workers and is applicable to any of the specialties of outpatient doctors. An exception to the rule is the position of a phthisiatrician. For him, the correction factor is 0.8.
The annual budget of the RVV is the amount of time a specialist works as a doctor in a year. When calculating the parameters of the annual budget of the RVV, vacation must be excluded.
Formula 2. Calculation of the annual budget of working time for the position of a doctor (B)
B = m x q - n - z, (2)
where B is calculated over a five-day work week.
m - number of workers. hours per day during daily work;
q - number of working days per year;
n - number of hours of reduced working time on weekends and before holidays;
z - number of workers hours during the holiday period.
As we can see, the results of the calculation of the planned function of the position of an outpatient doctor are directly related to the time limits for a visit, determined by Order No. 290n. This is true for any duration of labor leave, i.e., when using both basic and additional holidays. This means that the order definitely needs to be revised or supplemented to it so that the new norms for the admission of patients by doctors do not become an obstacle to the implementation of direct medical work.
The current stage of development of labor rationing in healthcare is characterized by two opposite trends:
- at the intersectoral level, a number of decisions are made aimed at creating a system of labor rationing, including in healthcare institutions; in one of the research institutes of the Ministry of Health of Russia, a division for labor rationing was opened medical workers;
- The Ministry of Health of Russia approves legal documents on labor that contain a lot of erroneous provisions, both editorial and semantic in nature, and do not correspond to the theory and practice of labor rationing.
1. Organizational technologies of labor rationing
As positive measures to create a system of labor rationing, one should recognize the approval of the Orders of the Ministry of Labor of Russia: dated May 31, 2013 No. 235 “On approval of methodological recommendations for federal bodies executive power on the development of standard industry labor standards” and dated September 30, 2013 No. 504 “On approval of guidelines for the development of labor rationing systems in state (municipal) institutions”.
Order No. 235 contains:
- conditions and terms for the revision of standard industry labor standards;
- normative factors;
- methods of labor rationing;
- labor intensity;
- stages of normative research work.
The appendix to the order provides statistical tools for the development of standard industry labor standards.
The main provisions of the order coincide with the methodological materials on labor rationing in the healthcare sector [ Shipova V.M. Fundamentals of labor rationing in health care ( tutorial) Under the editorship of Academician of the Russian Academy of Medical Sciences O P. Shchepin: - M .: GRANT Publishing House, 1998. - 320 p.; Labor rationing in health care, lectures No. 1-No. 10 M .: RIO FGBU "TsNIIOIZ", 2013-2017. ]. However, when applying Order No. 235, the specifics of the work of medical workers should be taken into account. IN Lately there is an increased interest of the heads of medical organizations in the development of local labor standards, including timing. In the process of timing, an examination of the volume and quality of work is carried out, an assessment of the compliance of medical and diagnostic measures with the diagnosis and state of health of the patient, and medical prescriptions. This work can only be carried out by an appropriate specialist who knows the technology of the diagnostic and treatment process well. It is a mistake to involve economists, personnel department employees, commissions in timing the activities of medical workers, since, firstly, these workers not only cannot conduct an expert assessment, but even accurately determine the name of the labor operation, and, secondly, the presence of persons who do not have a medical education is unacceptable when contacting a medical worker and a patient.

Order No. 504 defines the types of labor standards and establishes a connection between them. These provisions are of great importance to healthcare organizers and to all healthcare professionals. The fact is that the issues of labor rationing are still not included in the program of diploma and postgraduate training of doctors and paramedical workers, these issues are not considered in textbooks on public health.
Order No. 504 contains certain innovations in organizational technologies regulation of labor. The document provides recommendations for state (municipal) institutions on the development of the Regulations on the labor rationing system, which is either approved by the local normative act institutions, taking into account the opinion of the representative body of workers, or is included as a separate section in the collective agreement.
- labor standards applied in the institution;
- the procedure for implementing labor standards;
- the procedure for organizing the replacement and revision of labor standards;
- measures aimed at compliance with established labor standards.
The most important for medical organizations, taking into account the available regulatory framework on labor in the field of healthcare is the first section, in the annexes to which the following data are indicated:
- references to standard labor standards used in determining labor standards;
- the applied methods for determining the population rate based on the typical time rate, the number rate based on the typical service rate and the service rate based on the typical time rate (if calculations were made);
- calculation of the correction of standard labor standards, taking into account the organizational and technical conditions for the implementation of technological (labor) processes in the institution (if a correction was carried out);
- methods and means of establishing labor standards for individual positions (professions of workers), types of work (functions) for which there are no standard labor standards.
Order No. 504 also defines the circle of persons who should be involved in the development of a labor rationing system in an institution.

Taking into account the number of employees and the specifics of the activities of the institution for the performance of work related to labor rationing, it is recommended to create a specialized structural unit (service) for labor rationing in the institution. In its absence, the performance of work related to the regulation of labor may be entrusted to the structural unit (employee), which is in charge of staffing the activities of the institution, organization of labor and wages.
The implementation of these recommendations in medical organizations should be addressed, in our opinion, as follows. Taking into account the fact that medical workers do not possess, as indicated, the necessary knowledge and skills in labor rationing, the deputy chief physician for economic issues should be responsible for organizing labor rationing in medical organizations. In the absence of this position, the organization of labor rationing can be entrusted to the personnel department, accounting staff, while it should be emphasized that it is organization regulation of labor.
The direct development and establishment of labor standards on the basis of standard norms approved at the federal level, or in the absence of such, is carried out by the heads of structural medical and diagnostic units, chief and senior nurses, taking into account the specifics of the specific conditions of labor organization.
2. Analysis of the modern regulatory framework for labor in the healthcare sector
The labor standards of medical workers have been set out in recent years in the following departmental legal documents:
- orders of the Ministry of Health of Russia on the procedures for the provision of medical care;
- letters of the Ministry of Health of Russia on the formation and business case territorial program state guarantees free provision citizens of medical care for the corresponding financial year and planning period (hereinafter referred to as the territorial program);
- letters of the Ministry of Health of Russia, FFOMS "On methodological recommendations on methods of paying for medical care at the expense of compulsory medical insurance" (labor standards for dentistry).
The mass approval of the orders of the Ministry of Health of Russia on the procedures for the provision of medical care, an integral part of which are the recommended staffing standards, began in 2009 and, after a short break in 2014, continues to this day. To date, there are 67 orders. Unfortunately, the erroneous provisions of the labor standards given in these documents, as a rule, are not corrected during the revision, and in some cases new errors are added to them.
Systemic erroneous provisions of modern legal documents labor are reduced to the following.
2.1. Erroneous application of different types of labor standards

In health care, the following types of labor standards are used: norms of time, workload (service), number. The values of these indicators are presented in teaching materials on the regulation of labor in health care and, as indicated, in the order of the Ministry of Labor No. 504.
Time standards in health care are expressed in minutes, conventional units, conventional units of labor input (UUT), load (service) norms - in the number of visits per hour, year, patients per day, number of examinations, procedures per day, year or for any other period of time .
The size standards are presented in terms of the population or its contingents, the number of beds or round-the-clock posts per 1 medical position, the volume of a particular work.
In the orders for the procedures approved before 2012, the norms of time for visits in certain specialties were cited, erroneously called the norms of workload or workload. When reviewing such orders, these data are not indicated. However, in the current order for coloproctology (dated April 2, 2010 No. 206n), the time standards for a diagnostic and treatment appointment are given, called the load rate.
In the territorial programs, starting from 2008 and up to the present, a table is provided, the title of which indicates "the load indicator for 1 position of a doctor (middle medical worker)", and the content of the table shows the number of beds per 1 medical position and the number of beds per 1 post of nurses, i.e. population standards.
2.2. Unjustified change in the format of presentation of labor standards

The norms for the number of personnel in health care institutions are determined by the staffing standards used for medical workers, and the standard staffs used to standardize the work of employees and workers. medical organization. The difference between these documents is that staffing standards are set based on some indicator, for example, at the rate of 1 position of a general practitioner for 25 beds. The overwhelming majority of typical states do not require such a calculation, and one or another position is established for the presence or a certain capacity of an institution, unit, for example, the position of deputy chief physician for economic issues is established in a medical facility with 100 or more beds and including outpatient clinics. divisions.
The recommended staffing standards given in orders on procedures are modeled on model states that do not provide for calculation and are used for non-compliance. medical staff. With the transition to this new form of population norms, i.e. use instead staff standards typical states, the words so necessary for staffing standards have also disappeared: “the position is established on the basis of ...”, which can lead to different workloads for medical workers with the same amount of work. For example, if the position of a doctor is set as “1 for 20 beds”, this leads to the fact that only one position can be established for 20 beds, and for 30, and for 35 beds, which obviously leads to a different workload for the doctor. If the position was established “based on 20 beds”, as is customary in staffing standards, then 1.5 positions can be installed for 30 beds (30: 20 = 1.5), and 1.75 positions for 35 beds ( 35:20=1.75).
Only in two orders (dated November 15, 2012 No. 923n "Procedure for the provision of medical care in the field of "neurosurgery"" and dated November 15, 2012 No. 918n "Procedure for the provision of medical care to patients with cardiovascular diseases") and only in hospital departments of the position of medical workers are established "at the rate of 30 beds".
2.3. Violations of the nomenclature of medical organizations, specialties and positions of medical workers, hospital beds

Currently, the following legal documents on nomenclatures are in force:
- Order of the Ministry of Health of Russia dated 08/06/2013 No. 529n "Nomenclature of medical organizations";
- Order of the Ministry of Health of Russia dated 07.10.2015 No. 700n "Nomenclature of specialties of specialists with higher medical and pharmaceutical education" with additions made by order of the Ministry of Health of Russia dated 11.10.2016 No. 771n;
- Order of the Ministry of Health and Social Development of the Russian Federation of April 16, 2008 No. 176n with subsequent additions “Nomenclature of specialties for specialists with secondary medical and pharmaceutical education in the healthcare sector of the Russian Federation”;
- Order of the Ministry of Health of Russia dated December 20, 2012 No. 1183n “Nomenclature of positions of medical and pharmaceutical workers”;
- Order of the Ministry of Health of Russia dated October 08, 2015 No. 707n “Qualification requirements for medical and pharmaceutical workers With higher education in the direction of preparation “Health care and medical sciences””;
- Order of the Ministry of Health of Russia dated 10.02. 2016 No. 83n "Qualification requirements for medical and pharmaceutical workers with secondary medical and pharmaceutical education";
- Order of the Ministry of Health and Social Development of the Russian Federation of May 17, 2012 No. 555n "Nomenclature of the bed fund according to the profiles of medical care."
Compliance with these nomenclatures is mandatory for medical organizations. Incorrect names of positions and specialties in the staffing tables of medical organizations lead to complications in the provision of pensions for employees, the establishment of a work and rest regime, wages, and so on. Moreover, such violations are unacceptable in legal documents. However, in almost every order on orders there are names of positions and specialties that do not correspond to the current nomenclatures. So, for example, in orders on orders, the positions of a gynecologist are given instead of the position of an obstetrician-gynecologist, a dermatologist instead of a dermatovenereologist, a traumatologist instead of an orthopedic traumatologist, a neuropathologist instead of a neurologist, a laboratory assistant instead of a clinical doctor laboratory diagnostics, nurse ward instead of a ward (guard) nurse, a bacteriologist instead of a bacteriologist, a masseur instead of a massage nurse, etc., as well as positions that are not in the nomenclature, for example, a microbiologist, a senior laboratory assistant, a senior radiologist, etc. .
When applying orders on the nomenclature, one should keep in mind a number of existing contradictions between the nomenclature of positions, the nomenclature of specialties and qualification requirements. A number of medical positions indicated in the nomenclature of positions are not included in the nomenclature of specialties. These positions include: a diabetes doctor, a medical prevention doctor, a clinical mycologist, a laboratory mycologist, a palliative care doctor, a medical rehabilitation doctor. These positions are also absent in order No. 707n on qualification requirements, although for most of these positions there are labor standards defined in the relevant orders on procedures.
His "mite" in the incompatibility of orders on the nomenclature of specialties, positions and qualification requirements introduced the order of the Ministry of Health of Russia dated October 11, 2016 No. 771n, which included a number of specialties as an addition to the nomenclature of specialties of specialists with higher medical and pharmaceutical education.
These changes in the nomenclature of specialties are not accompanied by changes in either the nomenclature of positions or in the document on qualification requirements.
2.4. Erroneous data on the number of posts to ensure round-the-clock work

The organization of the activities of medical organizations involves different modes of operation of units and relevant positions for their functioning. So, for example, an ambulance station (department) operates around the clock; in a hospital to ensure round-the-clock provision of medical and diagnostic medical care, round-the-clock posts of middle and junior medical workers, a number of positions of doctors are established. The orders on procedures indicate the specific number of posts to ensure round-the-clock work: from 1 to 5.7 posts.
The number of posts to ensure round-the-clock work depends on two main groups of data:
- the number of working days and pre-holiday days in a year in which there are reductions in working hours;
- mode of work and rest positions.
The number of working and pre-holiday days in which there is a reduction in working hours changes annually.
The regime of work and rest differs not only in the names of positions, but even in the same position, but working in medical organizations in different regions of the country, for example, in an institution in the Central Strip of Russia and in the regions of the Far North due to different vacation duration.
Therefore, it is not a different number of posts to ensure round-the-clock work, specified in orders on procedures, that is erroneous, but the very indication in the normative record of this number of posts. The normative record on the staffing of round-the-clock work should contain only the number of beds for organizing this mode of operation, or a certain amount of work, for example, the number of emergency calls and, consequently, the number of teams. The specific number of positions must be calculated in a medical organization annually, depending on the mode of work and rest of the position and the number of working and pre-holiday days in the year in which there is a reduction in working time.
2.5. Unreasonable introduction of new indicators for labor rationing

When choosing an indicator for labor rationing, the following requirements must be observed:
- taking into account the current level of development and organization of medical care, labor organization, equipment, compliance with the relevant technologies of the treatment and diagnostic process;
- compliance with the degree of integration of the indicator to the conditions and nature of the work of a particular type of institution, ensuring the necessary accuracy in setting staffing standards; the influence of the main norm-forming factors and the need to take them into account in the normative indicator;
- coverage of the most common options for performing work, convenience for calculating staffing standards;
- the specific content of normative indicators, the possibility of establishing their quantitative value.
The following indicators meet these requirements:
- the number of the population or its individual contingents to establish the positions of outpatient doctors;
- the number of beds to establish the positions of medical workers in hospitals;
- the number of outpatient doctors and the number of beds or the amount of work to establish the positions of medical personnel of the auxiliary medical diagnostic service, most of the positions of middle and junior medical workers.
An unreasonable change in these indicators for the normalization of labor in the absence of their value fixed by statistics makes these data very manageable and leads to the possibility of an unjustified increase or decrease in the number of employees. An example of the erroneous introduction of a new labor indicator is the establishment in orders of orders of the position of an anesthesiologist-resuscitator for the number of workplaces of operating tables.
It is quite obvious that the number of workplaces, operating tables does not indicate the volume of work of the personnel, in this case it is necessary to determine at least the number of surgical interventions on one operating table, or the operating hours of the operating table, and so on. According to earlier orders of the USSR Ministry of Health, the standard number of these doctors was set to the number of surgical beds, and, in our opinion, there are no grounds for changing this indicator.
Another example of changing the indicator for labor rationing is to establish the standard number of nurse positions per office. In fact, the number of offices, as premises for the work of a doctor, is not in the statistics, and the indicator for the standard for the number of positions of a nurse should be the number of positions of a doctor of a particular specialty.
Another "novelty" of orders on orders is the change in the normative indicator for the position of chief physician, head of the department. Thus, the number of these positions in the children's polyclinic, according to the relevant order (dated April 16, 2012 No. 363n), is set for 10 thousand attached population. If we follow the "letter" of this order, then in a children's polyclinic serving 20,000 children, it is possible to establish 2 positions of chief physician, and 30,000 - 3 chief physicians, which is contrary to public health practice.
2.6. Lack of regulatory support for a number of departments of healthcare facilities, individual positions

In a number modern norms ative-legal documents turn out to be “missing” positions or entire divisions. So, the order on the order in the inpatient department of traumatology and orthopedics (dated March 31, 2010 No. 201n) did not provide for the positions of a dressing and operating room nurse. When this document was revised (No. 901n dated November 12, 2012), the position of a dressing nurse was introduced into the structure of this unit, and the position of an operating room nurse is still missing. In the staffing standards of the dermatovenerologic dispensary, there is no staffing of medical workers in the admissions department, in the staffing standards of the children's polyclinic - the security of the registry, etc.
2.7. Erroneous wording of the standard for the position of the head of the department
IN staffing in a medical organization, the position of head can be established only in the form of one position, although the procedure for establishing this position may be different: instead of the whole or part of the position of a doctor or in addition to medical positions. At the same time, the position of the head in outpatient departments is established by the number of positions of outpatient doctors of the corresponding specialty, in hospital departments - by the number of beds. In orders on orders, in some cases it is recommended to establish a fractional number of posts: 0.25; 0.5 or 0.75 posts.
The position of the head of the hospital department in a number of cases is established, as indicated, "based on 30 beds." Such a record is quite acceptable for most positions, but these positions include the head of the department. At the same time, it remains open question on the number of positions of managers in a department of a different capacity, for example, in a department with 45 or 50 beds. Following the specified standard, in a department with 45 beds, 1.5 positions of the head can be established (45:30 = 1.5), and in a department with 50 beds - 1.75 (50:30 = 1.667, rounded 1.75). Thus, the presented establishment of the positions of heads of departments is contrary to public health practice.
2.8. Inconsistency in the values of labor standards in different, simultaneously valid documents

In simultaneously acting orders on orders, a different standard is indicated for the same position. For example, the position of a surgeon, according to one of the orders, is set as 1 position per 10.0 thousand of the adult population, according to another - 0.65 positions. It is quite characteristic that both of these orders were approved in 2012 and entered into force almost simultaneously - in November-December 2012. The standard for the position of a pediatric urologist-andrologist has a two-fold difference: according to one of the orders on orders, this position is established for 10.0 thousand of the attached child population, according to another - for 20.0 thousand.
In addition to orders on orders, labor standards are also indicated in territorial programs, while for a number of profiles there is a discrepancy between these values and orders on orders. So, for otorhinolaryngology, according to the territorial program for 2016, a standard is set equal to 12 beds per 1 doctor's position, and according to the order on order - for 20 beds, for nephrology - for 12 and 15 beds, respectively, and so on.
There are no coincidences indicated in the territorial program and in the orders of the Ministry of Health, in terms of the standard labor costs for a visit: according to an order approved in mid-2015, the following standard time standards for a visit were established: for a district general practitioner - 15 minutes, for a doctor general practice(family doctor) - 18 min. The territorial program for 2016 states the following: “The recommended time limit for 1 visit to a district therapist, general practitioner, district pediatrician is an average of 20 minutes.”
Such conflicting data on the value of standard labor indicators specified in simultaneously valid legal documents approved by the same department require urgent action at the federal level of health management.
2.9. Recommendations for the use of one indicator out of several given in the standard
In staff standards, the establishment of a particular position is possible for several indicators. In these cases, the number of posts is calculated for each indicator, and then the calculated number of posts is summed up. In the orders on procedures approved in 2016 (dated March 1, 2016 No. 134n, dated March 24, 2016 No. 179n), the union "or" is included in the normative record. This union is used in Russian to connect two or more sentences, as well as homogeneous members of a sentence that exclude each other. Thus, the normative record with the union "or" suggests that you need to choose only one of the given indicators. However, the logic and practice of applying labor standards suggests that if a position in one of the medical organizations is set for one of the indicated indicators, for example, in one of the medical and physical education clinics for the number of people involved in sports, and in another - for another indicator, for example, on the urban population living on the territory of the dispensary, this will lead to a different standard number of positions that does not reflect the full scope of work and the load on servicing all the contingents of the population and athletes indicated in the document.
2.10. Economic groundlessness of new labor standards

All the shortcomings of legal documents indicated in the previous paragraphs can be considered as editorial, although they are unacceptable in documents of this kind. If desired, erroneous provisions can be corrected: you can enter calculation method the formation of labor standards, bring the names of positions, specialties in line with the nomenclatures, change the regulatory records for establishing the positions of heads of departments, set the required indicator for round-the-clock work, eliminate contradictions in simultaneously acting legal documents, and so on.
The medical and economic assessment of modern labor standards was carried out according to the methodology of labor rationing in healthcare. Within the framework of this publication, it is not possible to describe all the methodological approaches used, they are presented in sufficient detail in the relevant literature and are used in medical organizations with economic analysis activities of medical workers and departments.
Carrying out calculations of the normative number of medical positions only according to orders approved over the past two years (except for order No. 134n), showed that over 30 thousand additional positions are needed for their implementation, including the need to increase the positions of narcologists by more than 3 times compared to their actual number, geriatricians - 10 times and so on. Moreover, the calculations were carried out only on those indicators that have statistical security.
A striking example of the economic groundlessness of labor standards is Order No. 134n “On approval of the procedure for organizing the provision of medical care to persons involved in physical culture and sports (including in the preparation and holding physical culture events and sports events), including the procedure for medical examination of persons wishing to undergo sports training, engage in physical culture and sports in organizations and (or) fulfill the test standards (tests) of the All-Russian Physical Culture and Sports Complex "Ready for Labor and Defense"".
If, when calculating the normative number of medical positions, only one indicator is used: the number of people involved in sports and health clubs, organizations and groups, which is currently 39071.4 thousand people [ Healthcare in Russia, 2015: Stat. Collection / Rosstat. - M., 2015. - 174 p.], i.e., contrary to common sense, to use the word “or” indicated in the regulatory record, it turns out that in order to implement only this provision of the order, the number of medical posts is required that exceeds the actual number of all doctors in the country. For comparison, we note that the previous order (dated August 9, 2010 No. 613n) established the standard number of doctors in sports medicine and physiotherapy equal to more than 25 thousand positions, and the actual number of these doctors is 3.9 thousand positions. Moreover, these positions include not only doctors working in medical and physical education dispensaries, but also in hospitals, sanatoriums, and clinics. Under these conditions, with such insecurity of staff standards current order the very decision to revise the legal document is erroneous.

With regard to the normative number of middle and junior medical workers, a different trend is revealed: a decrease in the number of middle medical personnel and the disappearance of the norm for the number of junior medical workers. In accordance with the new order (dated 05.05.2016 No. 279n), the standard for the positions of paramedical workers in sanatorium-and-spa organizations has been reduced tenfold compared to those previously in force, and the standard for the position of a ward nurse (according to the nomenclature in force during the period of approval of this standard) or the standard for junior there is no nurse to care for the sick (according to the current nomenclature) at all.
The introduction of order No. 279n of the Ministry of Health of Russia into healthcare practice does not allow organizing the work of a sanatorium for children with less than 250 beds and a sanatorium for adults with less than 500 beds, primarily because of such a reduction in the standard number of middle and junior medical workers and the impossibility of their round-the-clock work. In sanatoriums of greater capacity, a reduction in the number of round-the-clock posts of ward nurses (guards) and a complete lack of standard provision of junior medical workers will lead to significant difficulties in organizing the provision of medical care.
There are no standards for the positions of orderlies in the recommended staffing standards for the department (office) of medical prevention for adults (dated September 30, 2015 No. 683n), the audiology room (dated April 9, 2015 No. 178n), the geriatric department and the geriatric office (order No. 38 dated January 29, 2016 ) and so on.
The reduction in the actual number of junior medical personnel in medical organizations is due to an attempt in this way to fulfill the May 2012 decrees of the President of Russia. In medical organizations, the positions of nurses are being transferred to the positions of cleaners, i.e., these positions are being excluded from the number of medical workers, and in a few months of 2016, according to Rosstat, about 50 thousand nurses quit [ Chief Nurse, 2016. - No. 10. - P.8.]. It should be noted that such a transfer is not always justified, since in a number of cases the nurse performs not only the functions of a cleaner, but also takes part in providing medical care to the patient to a certain extent, i.e., performs the functions of a junior nurse to care for the sick, especially in the provision of hospital and sanatorium care. But in this case, we are talking about the standard provision of junior medical personnel, and in order to transfer the positions of nurses to the positions of cleaners, it is necessary to have a standard for the position of a nurse. In this regard, we consider it erroneous to exclude the positions of junior medical personnel from staff standards.
Conclusion

The current stage in the development of labor rationing can be viewed as a transition to the creation of a system of labor rationing. The measures taken to create this system are apparently not enough, since legal documents containing such obvious errors are still being approved.
The critical mass of erroneous provisions of orders on procedures in terms of labor standards, the main of which is economic unreasonableness, determines the need to revise these legal documents. IN modern conditions organization of labor rationing and functioning in one of the research institutes of the Ministry of Health of Russia of the labor rationing unit, all documents of this kind should be developed jointly with specialists in labor rationing, or at least undergo an appropriate peer review before they are approved. Such work is partially carried out, but, in our opinion, it should be extended to all draft legal documents on labor standards.
In order to improve the development of labor standards, it is necessary to include labor rationing issues in the training program for doctors and paramedical personnel and postgraduate training in the specialty "Organization of health care and public health", "Organization of nursing", holding seminars, lectures on this topic, and, first turn, for the developers of labor standards and specialists who approve these standards.
For chief physicians, heads of departments of medical organizations, representatives of ministries and departments in the field of healthcare: we suggest that you familiarize yourself with the program of the symposium, which will be held on August 21 - 25, 2017 "Management of a medical institution in modern conditions" .
We invite you to take part in the International Conference for Private Clinics , where you will get the tools to create a positive image of your clinic, which will increase the demand for medical services and increase profits. Take the first step towards the development of your clinic.
All rights reserved. When reprinting materials, an active link to the article is required.
Management of the organization of labor in any enterprise (organization) is carried out by planning to improve the organization of labor , which is part of the economic planning of its activities, and the strict implementation of the planned activities.
Market relations not only do not negate the need for planning within enterprises, but also increase its importance. Planning is preceded by an analysis of the level of labor organization and the identification on its basis of weak links in the organization of labor.
The main requirement for such planning in a medical institution is the maximum specificity and validity of each stage of work.
And of course, the planning of measures to improve the organization of labor should be based on a clear system of norms (standards) and scientific organization of labor (NOT).
Rationing is an essential element of labor organization , the essence of which is to determine objectively necessary costs working time when designing rational labor processes and establishing progressive, scientifically based labor standards.
The system of labor standards promotes the best use of material and labor resources, since it is the fundamental principle of the organization of labor and is determined on the basis of one or more labor standards.
The following labor standards (standards) apply in healthcare .
Norms of time - this is the regulated duration of the performance of a unit of work by personnel or a group of employees in typified organizational and technical conditions of activity. Time norms are expressed in minutes, hours, conventional units, conventional units of labor input (UET).
Load (maintenance) rates - the established amount of work performed per unit of time by personnel or a group of personnel in specific organizational and technical conditions of activity. Load (service) rates are expressed in the number of visits per hour, shift, year; the number of patients served per day; number of studies, procedures per hour, shift, month, quarter, year or other period of time.
Number standards (staff standards) - the necessary number of personnel to perform all the functions assigned to the institution (department) and a certain amount of work, established according to standard indicators and their combinations, calculated values.
Number standards in health care are drawn up in the form of staffing standards or model states. The main indicator and measure for establishing the positions of medical personnel in outpatient clinics is the population or its individual contingents, for hospitals - the number of beds.
At the same time, at the intersectoral (for staff of employees and workers of healthcare facilities) and industry levels for different groups personnel, different types of labor standards are established.
So for the main staff of outpatient clinics or departments, there are all three types of standards, for the main staff of hospital institutions (divisions), ambulance stations - only numbers.
For the personnel of the auxiliary medical and diagnostic service, employees and workers of medical institutions in without fail norms of time and norms of numbers.
The norms of time for certain types of work for personnel, employees and workers of health care institutions are determined, as a rule, according to documents approved at the intersectoral level. Moreover, the prescription of the approval of these documents casts doubt on their relevance.
For other groups of personnel, the norms of time for certain types of work are not approved at the federal level, except for the provision of outpatient dental care.
Conventional units for accounting for the labor intensity of dentists and dentists were approved by order of the USSR Ministry of Health of January 25, 1988 No. 50 “On the transition to a new system for recording the work of dentists and improving the form of organizing a dental appointment.” In the future, these norms were revised many times, mainly in the direction of increasing the classifier's occupancy. medical services.
The transition to a new indicator for standardizing the work of dentists (individual services instead of the generally accepted indicator for outpatient doctors - visits) is, according to experts, erroneous, since in the absence of fixing the volume of these services in the reporting accounting documentation this can lead to inflated financial claims for dental care.
Workload (service) standards are set at the federal level for two groups of personnel: outpatient doctors and partly for medical personnel of the auxiliary medical and diagnostic service.
For outpatient doctors, the workload (service) rates in the form of the number of visits per 1 hour of admission were approved by the order of the USSR Ministry of Health dated September 23, 1981, No. 1000 “On measures to improve the organization of the work of outpatient clinics”.
Subsequently, in connection with the expansion of the rights of chief physicians, by order of the USSR Ministry of Health of July 22, 1987, No. 902 “On the abolition of planning and evaluation of the work of outpatient clinics by the number of visits”, these calculated service standards for doctors of outpatient clinics were recognized as invalid . However, in the absence of other officially approved indicators, they continue to be used in healthcare practice.
The load (service) norms for some groups of medical personnel of the auxiliary medical and diagnostic service in the form of the number of manipulations, procedures per day are given in a number of orders according to time standards.
Improving the organization of work in healthcare institutions requires further development of the methodology for determining the norms of time for medical services, methods for calculating the norms of the workload of medical personnel, approaches to determining and planning the number of medical personnel.
For this it is necessary to solve the following tasks :
- formation new system regulation of the work of medical personnel using world standards on technologies for the provision of medical services;
- development modern techniques according to the calculation of the norms of time (labor intensity of work) for the provision of simple and complex medical services;
- formation of a methodology for calculating the load norms of medical personnel of health care institutions in the following areas: outpatient reception, diagnostic services, hospitals. This should take into account development priorities Russian healthcare in modern conditions;
- development of new approaches to determining and planning the number of medical personnel of health care institutions.
Ways to improve the organization of labor based on a rationing system lead through the systematic and consistent implementation of the principles of the scientific organization of labor (NOT) .
A scientific approach to the organization of labor makes it possible to combine technology and people in the best possible way, ensures the most efficient use of material and financial resources, reducing labor intensity and increasing labor productivity. It is aimed at preserving the health of workers, enriching the content and humanizing their work.
The scientific organization of labor in healthcare institutions is as follows :
- Regulation labor functions based job descriptions . Work in this direction involves a periodic review of the established organizational schemes for the work of medical staff, replacing them with more advanced and rational forms of distribution of labor functions.
- Centralization of medical-diagnostic, auxiliary economic services and restructuring of the work of these services "into departments".
- Improving the forms of medical documentation and methods of its maintenance, the use of organizational intra-institutional communication systems.
- Rational organization of workplaces (equipment and layout, creation of hygienic comfort and aesthetic working environment).
- Improving socio-psychological relations in healthcare institutions. This is an important element of NAT as applied to the work of medical workers. Important role at the same time, such organizational measures as material and moral stimulation labor, planning social development team, improving the style and methods of leadership, using the educational power of traditions.
The introduction of recommendations to improve the organization of labor in the practice of health facilities, as a rule, is associated with the need to use technical means- office equipment, new modern equipment, intra-institutional communications, etc.
At the same time, it becomes necessary to develop organizational and technical projects, it is often necessary to reconstruct mass-produced devices in relation to the specific conditions of medical institutions, and sometimes create samples of non-standard office equipment.
So, it is obvious that only management organized on scientific basis, will allow finding optimal solutions for many of the problems that arise in a rapidly changing economic conditions, can contribute effective work medical personnel.
List of sources used
- Androsova L.A. Labor Economics: textbook. federal agency of Education. Penza State University, 2005. - 160p.;
- Ashirov R.Z. Economics and organization of healthcare: a textbook. - Saransk: Red October, 2002. - 250 p.;
- Genkin B.M. Economics and sociology of labor: Textbook for universities - 5th ed. / B.M. Genkin. - M.: Norma, 2006. - 343 p.;
- Kravchenko A.I. History of management. 5th ed. - M.: Academ. Project: Tricksta, 2005 - RGIM Library [electronic resource] - access mode: ttp://www.i-u.ru;
- Medical management. 2011. [electronic resource] - access mode: http://handbooks.ru;
- Rofe A.I. Labor Economics: textbook - M.: KNORUS, 2010 - 400 p.;
- Shipova V. M. Labor rationing as a system of support for personnel decisions in healthcare institutions / Directory of personnel officer. 2009. - No. 4.;
2012-2015 Lana Zabrodskaya (on Google+). When copying materials from this site link to the source is required
8 . 499 . 138 . 51 . 34
119331 Moscow,
st. Maria Ulyanova, 9, bldg. 1


![]()

Modern approaches to labor rationing in medical organizations
Organization of labor rationing in medical organizations
A number of provisions of the order correspond to the methodology of labor rationing used in the healthcare sector, however, the document also introduces certain changes in the organization of labor rationing in medical organizations.
The order provides the following definitions of the basic labor standards:
Norms of time - the cost of working time for the performance of a unit of work (function) or the provision of services by one or a group of employees of the appropriate qualification;
Service rates - the number of objects (jobs, equipment, areas, etc.) that an employee or a group of employees of appropriate qualifications are required to service during a unit of working time;
Number norms - the established number of employees of a certain professional and qualification composition, necessary for the implementation of specific production, managerial functions or scope of work.
These definitions are traditionally used in healthcare as well. Time norms are expressed in minutes, conventional units, conventional units of labor input (UET).
For example, the standard cost of a doctor's working time per visit is 15 minutes, the standard cost of a massage nurse for massage of an infant is 3 massage units.
Load (service) rates are expressed in the number of visits per hour, year (planned function of a medical position), patients per day, number of studies, procedures per day, year, or for any other period of time. For example, 4 visits per hour for an outpatient doctor, 20 patients per day for a hospital doctor.
Number norms are expressed in health care in the form of staffing standards and model states. Staff standards are used for medical personnel, while the calculation method for the formation of labor standards is used.
Model states are used for non-medical personnel, while, as a rule, no calculations are required, and the standard is set for an institution or unit of a certain capacity.
The norms for the number of outpatient doctors are expressed in the number of medical positions per 10.0 thousand of the population or its contingent, for example, 5.9 positions of a district general practitioner per 10.0 thousand of the adult population; or in population per 1 position, for example 1 position of an obstetrician-gynecologist for a certain number of women.
The norms for the number of medical workers in hospital units are established based on the number of beds per 1 position or 1 round-the-clock post.
The analyzed order notes that in the absence of standard labor standards for certain types of work and workplaces, the relevant labor standards are developed in the institution, taking into account the recommendations of the organization exercising the functions and powers of the founder, or with the involvement of relevant specialists in the prescribed manner.
Analysis of the labor process based on the standard for the provision of state (municipal) services, dividing it into parts;
The choice of the optimal variant of technology and organization of labor, effective methods and techniques of work;
Designing modes of operation of equipment, techniques and methods of work, systems for servicing workplaces, modes of work and rest;
Determination of labor standards in accordance with the characteristics of technological and labor processes, their implementation and subsequent adjustment as the organizational and technical conditions for the implementation of technological (labor) processes change.
When carrying out this work, it is recommended to focus on guidelines for federal executive authorities on the development of standard industry labor standards, approved by Order No. 235, in terms of organizing work and calculating labor standards.
In particular, in state (municipal) institutions, it is recommended to develop a regulation on the labor rationing system, which is either approved by the local regulatory act of the institution, taking into account the opinion of the representative body of workers, or included as a separate section in the collective agreement.
Labor standards applied in the institution;
The procedure for the implementation of labor standards;
The procedure for organizing the replacement and revision of labor standards;
Measures aimed at compliance with established labor standards.
The most important and relevant for medical organizations is the first of these sections. The appendix to this section contains:
Applied methods for determining the population rate based on the typical time rate, the number rate based on the typical service rate and the service rate based on the typical time rate (if calculations were made);
Calculation of the correction of standard labor standards, taking into account the organizational and technical conditions for the implementation of technological (labor) processes in the institution (if a correction was carried out);
Methods and ways of establishing labor standards for individual positions (professions of workers), types of work (functions) for which there are no standard labor standards.
Order No. 504 recommends providing for a period for conducting an analysis to determine the advisability of revising the applicable labor standards at least once every five years. Based on the results of the analysis, a decision can be made to maintain the established labor standards or to develop new standards.
Until the introduction of new labor standards, the previously established ones continue to apply. The inconsistency, as mentioned, of the current legal and regulatory framework for labor in the healthcare sector determines the need to turn to regulatory documents 30-40 years ago, which in some cases do not correspond to the technology of the diagnostic and treatment process.
At the same time, the main labor operations of the attending physicians of hospitals, outpatient clinics and their structure have not undergone significant changes.
This is evidenced by the results of chronometric observations conducted in 2013 of the activities of doctors in the provision of primary health care.
At the same time, an increase in the volume of diagnostic studies, and most importantly, the provision of modern equipment to medical organizations, conflicts with the time standards for diagnostic studies, developed and approved 20-30 years ago.
At the sectoral level, work on the revision of labor standards is not carried out.
The development of labor standards directly in a medical organization is a very laborious work that requires special training. In these cases, it is advisable, in our opinion, to use the provision of Order No. 504 on the introduction of correction factors for labor standards.
An important provision of Order No. 504 is the definition of the circle of employees for the organization of labor rationing.
The document states that the development (definition) of a labor rationing system in an institution should be carried out by specialists with the necessary knowledge and skills in the field of organization and labor rationing.
Taking into account the number of employees and the specifics of the activities of the institution for the performance of work related to labor rationing, it is recommended to create a specialized structural unit (service) for labor rationing in the institution. In its absence, the performance of work related to the regulation of labor can be assigned to a structural unit (employee), which is in charge of staffing the activities of the institution, organization of labor and wages (see materials in the ES "Economics of LPU" - get access> 9gt;) .
Responsible for the organization of labor rationing in medical organizations should be, in our opinion, the deputy chief physician for economic issues.
However, this position is not available in all medical organizations. In this case, the responsibility for organizing labor rationing can be assigned to an economist, deputy chief physician for personnel, head of the personnel department, personnel specialist, chief accountant.
However, in all cases, it is necessary to involve specialists, organizers of medical care, and, above all, deputies of the chief physician for medical affairs, heads of medical and diagnostic units, in the regulation of labor in medical organizations. This is due to the fact that only these specialists, who know the technology of the treatment and diagnostic process, can conduct an expert assessment of the quality and volume of medical care necessary for the development of labor standards.
The Labor Code establishes the obligation to keep records of the time actually worked by each of the employees. This is an important point in respecting their rights - after all, overtime work, work at night or on weekends, non-working holidays should be compensated. Doctors are a special category of workers: their processing can affect the quality of services provided to the population. Therefore, the employer must strictly comply with the requirements of labor legislation regarding the duration of the work of physicians. Today we will tell you what types of working hours are possible for medical workers, how many hours a week they should work, according to what forms of documents it is necessary to keep records of actually worked time.
General information about working hours
Working time is the time during which the employee, in accordance with the internal labor regulations and conditions employment contract must perform labor duties, as well as other periods of time that, in accordance with the Labor Code of the Russian Federation, other federal laws and other regulatory legal acts of the Russian Federation relate to working time (special breaks for heating and rest - Article 109 of the Labor Code of the Russian Federation, additional breaks for feeding a child - Article 258 of the Labor Code of the Russian Federation, etc.). The normal duration of such time cannot exceed 40 hours per week.
For medical workers Art. 350 of the Labor Code of the Russian Federation establishes a reduced working time, which is normal for them - 39 hours a week. Also, depending on the position or specialty, the working hours of doctors are changed by the Government of the Russian Federation.
For your information. Article 92 of the Labor Code of the Russian Federation establishes a reduced working time for workers under the age of 16 - no more than 24 hours a week, from 16 to 18 - no more than 35 hours a week, workers who are disabled groups I or II - no more than 35 hours , and for persons employed in work with harmful and (or) dangerous working conditions - no more than 36 hours.
In particular, on the basis of Decree of the Government of the Russian Federation of February 14, 2003 N 101, the following working hours are established:
1. 36 hours a week - for doctors, paramedical and junior medical personnel:
— infectious diseases hospitals;
— skin and venereal dispensaries, leper colonies, medical facilities for the prevention and control of AIDS;
— laboratories that diagnose HIV infection;
- psychiatric (psycho-neurological), neurosurgical, narcological health facilities intended to serve citizens suffering from mental illness;
- children's psychiatric (psycho-neurological) health facilities, educational institutions for mentally retarded children;
— physiotherapy facilities;
— public service medical and social expertise, carrying out examination of citizens suffering from mental illness;
- stations (departments) of emergency and emergency medical care, regional, regional and republican hospitals.
2. 33 hours a week:
- for doctors of healthcare facilities (outpatient clinics, dispensaries, medical centers, stations, departments, offices) to conduct only outpatient admission of patients;
– doctors and paramedical personnel of physiotherapeutic treatment facilities and offices with a full working day on medical generators "UHF" with a power of over 200 W;
— dentists, orthopedic dentists, dentists-therapists, dentists and technicians (except for dentists-surgeons) of dental health facilities and offices.
3. 30 hours a week for doctors, paramedical and junior medical personnel:
— tuberculosis and anti-tuberculosis organizations (their structural divisions), institutions social services population intended to serve patients with tuberculosis;
- bureau of forensic medical examination, pathological and anatomical departments, laboratories, mortuaries directly working with corpses and cadaveric material;
- institutions of the state service of medical and social expertise that carry out examination of citizens with tuberculosis;
- health care organizations when working on the procurement and conservation of cadaveric blood;
- when working with gamma therapy and experimental gamma radiation in wards for patients with imposed radioactive preparations, work related to gamma installations;
- when working with X-ray diagnostics, fluorography, on a rotational X-ray therapeutic unit with visual control.
Note. Nurses of x-ray, fluorographic rooms and installations should work 30 hours a week, helping the doctor with x-ray diagnostics and fluorography for at least half of the working day.
4. 24 hours a week - for medical workers who directly carry out gamma therapy and experimental gamma irradiation with gamma preparations in radio manipulation rooms and laboratories.
Working hours
Health workers may work in various modes- 5-day work week with two days off, irregular working hours, shift work, part-time work, etc.
The establishment of a working regime is important from the point of view of the distribution of the norm of working hours during the accounting period - a week, month, quarter or year. For example, with a 40-hour week, the duration daily work(shifts) should not exceed 8 hours per day. And how to determine the duration of daily work (shift) with a reduced working time? The Order of the Ministry of Health and Social Development of the Russian Federation dated August 13, 2009 N 588n will help us with this. In particular, to determine the duration of the shift (daily work), it is necessary to divide the established duration of the working week by 5 days (paragraph 1). Accordingly, the duration of the shift of health workers will be:
- with a 39-hour work week - 7.8 hours;
- at 36-hour - 7.2 hours;
- at 33 hours - 6.6 hours;
- at 30 hours - 6 hours;
- at 24-hour - 4.8 hours.
To calculate the norm of working time for an accounting period, for example, a month, it is necessary to divide the working week by 5 (working days in a week) and multiply by the number of working days according to the calendar of the 5-day working week of this month. From the result obtained, it is necessary to subtract the hours by which working time is reduced on the eve of non-working holidays. For example, the norm of working hours for December 2013 will be: (39 hours / 5 days) x 22 days. - 1 hour = 170.6. 39 hours is the normal duration of work for a medical worker, 22 is the number of working days in December, 1 hour is the time by which the shift preceding January 1 (a public holiday) is reduced.
In addition to such a calculation of the duration of daily work, it is worth considering the requirements Labor Code, the norms of which have already determined the maximum duration of work for:
- employees aged 15 to 16 years - 5 hours, from 16 to 18 years - 7 hours;
– students of general educational institutions, educational institutions of primary and secondary vocational education, combining during school year study with work, at the age of 14 to 16 years - 2.5 hours, from 16 to 18 years - 4 hours;
- disabled persons - in accordance with a medical certificate issued in accordance with the procedure established by federal laws and other regulatory legal acts.
If the physician is busy hazardous work or work with hazardous working conditions, where a reduced working time is established, the maximum allowable duration of daily work (shift) cannot exceed:
- with a 36-hour work week - 8 hours;
- with a 30-hour work week or less - 6 hours.
By virtue of Art. 94 of the Labor Code of the Russian Federation, the duration of daily work (shift) in comparison with that established for persons employed in work with harmful and (or) dangerous working conditions may be increased by a collective agreement, subject to the maximum weekly working hours and hygienic standards of working conditions.
note! The duration of the working day or shift immediately preceding a non-working holiday is reduced by 1 hour, and if the employer has a 6-day working week, this duration cannot exceed 5 hours (Article 95 of the Labor Code of the Russian Federation).
Duration of work (shift) at night on the basis of Art. 96 of the Labor Code of the Russian Federation is also subject to reduction. But it can be equal to the duration of work in the daytime in cases where it is necessary for working conditions, as well as in shift work with a 6-day working week with one day off. The list of the specified works can be determined by the collective agreement, the local normative act.
Now let's move on to working hours.
In medical institutions, the following working hours are most often established:
1. Shift work - work in 2, 3 or 4 shifts. This mode is introduced in cases where the duration production process exceeds the allowable duration of daily work, as well as in order to more efficiently use equipment, increase the volume of products or services provided (Article 103 of the Labor Code of the Russian Federation). Usually, a shift regime is established at ambulance stations, in emergency medical care departments of medical institutions, medical institutions that provide emergency specialized (sanitary and aviation) medical care. As you know, such units work around the clock. The duration of the shift in this case can be 8 hours for a three-shift mode of operation or 12 hours for a two-shift mode. The main thing is that the norm of working hours for a month, quarter or year is observed.
During shift work, each group of employees must perform duties during the established working hours in accordance with the shift schedule, which is adopted taking into account the opinion of the representative body of employees and is brought to the attention of the staff no later than 1 month in advance.
The schedule is developed in such a way that the physician, having worked one shift, goes on vacation, after which he will work on another shift. Sometimes the work schedule is tied to the dates of the month or days of the week: for example, Monday, Wednesday, Friday - the first shift, Tuesday, Thursday, Saturday - the second.
Please note that a month's work hours may not match the normal number of hours worked in the same period if the schedule is quarterly, half-yearly or yearly. For example, if the norm of hours for a health worker in the IV quarter of 2013 is 467 hours, he can work like this:
The table shows that despite the discrepancy for individual months of the normal number of working hours to the number of working hours according to the schedule, in general, the entire norm of time was worked out for the accounting period.
Quite often, medical workers work according to the schedule every three days or the first shift on even days of the month, the second - on odd ones. Is this work shift? No, this mode of operation is not interchangeable, although schedules are also drawn up for it. It's more of a flexible schedule.
2. Flexible working hours. This mode of operation is referred to in Art. 102 of the Labor Code of the Russian Federation. In particular, under this regime, the beginning, end or total length of the working day (shift) is determined by agreement of the parties. At the same time, the employer must ensure that the employee works out the total number of working hours during the relevant accounting periods (working day, week, month, etc.). Recall that the norm of working time for a month, quarter, half a year or a year is calculated in accordance with the Order of the Ministry of Health and Social Development of the Russian Federation of August 13, 2009 N 588n.
3. Home duty - the stay of a medical worker of a medical organization at home waiting for a call to work (to provide medical care in an emergency or urgent form).
When taking into account the time actually worked by an employee of a medical organization, the time on duty at home is taken into account in the amount of 1/2 hour of working time for each hour of duty (Article 350 of the Labor Code of the Russian Federation). The total duration of the working hours of a medical worker, taking into account the time of duty at home, should not exceed the norm of working hours for the corresponding period.
In addition, for certain categories medical workers may apply other modes of operation.
Part-time work. Article 93 of the Labor Code of the Russian Federation determines that, by agreement between an employee and an employer, a part-time (shift) or part-time working week can be established both at the time of employment and subsequently. That is, the employee will work not 5 days a week, but, for example, 3, or the duration of his working day will not be 7.2 hours, but 5.
Note that the employer will not be able to refuse to establish such a working regime for a pregnant employee, as well as an employee if he:
- one of the parents (guardians, trustees) who has a child under the age of 14 (a disabled child under the age of 18);
- a person caring for a sick family member in accordance with a medical report.
The remuneration of an employee working part-time is made in proportion to the time worked by him or depending on the volume of work performed by him. At the same time, such work does not entail any restrictions for employees on the duration of the annual basic paid leave, the calculation of seniority and other labor rights.
Irregular working hours. This is a special mode of work, in accordance with which individual employees may, by order of the employer, if necessary, be occasionally involved in the performance of their labor functions outside the working hours established for them. But this mode of operation can not be established by any health worker. The list of positions of employees with irregular working hours is established by a collective agreement, agreements or local regulations adopted taking into account the opinion of the representative body of employees, and usually it includes heads of medical institutions - chief doctors and their deputies, as well as senior nurses.
Pay attention to the fact that under any mode, a medical employee may have overtime work - overtime.
Time tracking
Since the payroll also depends on the hours actually worked (for example, for overtime work or work at night), and the provision of certain guarantees and compensations (for example, milk is issued only on days of actual employment at work with harmful conditions labor), it is important to keep a record of it.
Order of the Ministry of Finance of the Russian Federation of December 15, 2010 N 173n approved the forms of time sheets that medical institutions should use to record working time:
- form 0301008 - time sheet;
- form 0504421 - timesheet and payroll.
The report card in the form 0504421 is maintained by persons appointed by order for the institution, monthly for the whole medical institution or in the context of structural divisions (departments, departments, faculties, laboratories, etc.), separate subdivisions(branches). The time sheet is opened monthly 2-3 days before the start of the billing period based on the time sheet for the previous month.
note! In the time sheet of form 0504421, only cases of deviations from normal use working hours established by the internal labor regulations. In the upper half of the line, for each employee who had deviations from the normal use of working hours, the hours of deviations are recorded, and in the lower half - the legend of deviations. At the bottom of the line, hours of operation during the night are also recorded.
If one employee has medical institution two types of deviations in one day (period), the lower part of the line is written as a fraction, the numerator of which is the symbol of the type of deviations, and the denominator is the hours of work. If there are more than two deviations in one day, the name of the employee in the report card is repeated.
Recall that the marks in the report card about the reasons for absenteeism, part-time work or work outside the normal working hours are made on the basis of duly executed documents (sick leave certificate, certificate of fulfillment of state or public duties, written warning of downtime, written consent of the employee to work overtime in cases established by law, etc.).
At the end of the month, the employee responsible for maintaining the time sheet in the form 0504421 determines the total number of days (hours) of absences, as well as the number of hours by type of overtime (substitution, work on holidays, work at night, etc.) with their entry in the appropriate columns (35, 42, 43, 45, 47, 49, 51). The completed time sheet is signed by the person entrusted with its maintenance.
For your information. The time sheet of form 0301008 actually repeats the form of the time sheet T-13, approved by the Decree of the State Statistics Committee of the Russian Federation of 01/05/2004 N 1. Some institutions do not apply this form, referring to the said resolution, in accordance with clause 2 of which this form budget institutions does not apply. However, before the adoption new form timesheets for state (municipal) institutions, a timesheet of form 0301008 can also be used.
The completed time sheet is submitted to the accounting department for settlements in the appropriate columns. After approval by the head of the institution, the time sheet is used to compile the payroll (f. 00504401) or payroll (f. 0301010).
Summarized accounting of working hours
In textbooks and articles in the media, you can read that accounting for working time can be daily (the number of days worked per month is subject to accounting, since the duration of work is the same, and work in excess of this duration is recognized as overtime), weekly (applies if, depending on the specifics of work only its weekly duration can be observed, and the time of daily work or shift is regulated by the schedule) and summarized. The first two types are not regulated by law, but let's talk a little more about the summarized accounting.
Note. In the case of summarized accounting of working time, the accounting period cannot exceed one year.
The summarized accounting of working time is introduced when, according to the conditions of production (work) in the institution as a whole or when performing certain types work, the daily or weekly working hours determined for this category of workers cannot be observed (Article 104 of the Labor Code of the Russian Federation). When establishing such an accounting regime, it must be remembered that the length of working time for the accounting period (month, quarter and other periods) should not exceed the normal number of working hours. The accounting period cannot exceed 1 year.
The normal number of working hours for the accounting period is determined on the basis of the weekly working hours established for this category of employees. For persons working part-time (shift) and (or) part-time working week, the normal number of working hours for the accounting period is reduced accordingly.
The procedure for introducing the summarized accounting of working hours is established by the internal labor regulations and is mainly relevant where there is shift work or flexible working hours.
Active Edition from 02.10.1987
| Document name | LETTER of the Ministry of Health of the USSR dated 02.10.87 N 02-14 / 82-14 "ON THE PROCEDURE FOR EXPANDING INDEPENDENCE AND INCREASING THE RESPONSIBILITY OF THE HEADS OF HEALTH CARE AUTHORITIES WHEN APPLYING THE ORDER OF THE MINISTRY OF HEALTH OF THE USSR OF AUGUST 13, 1987 N 955" |
| Document type | letter, guidelines |
| Host body | Ministry of Health of the USSR |
| Document Number | 02-14/82-14 |
| Acceptance date | 01.01.1970 |
| Revision date | 02.10.1987 |
| Date of registration in the Ministry of Justice | 01.01.1970 |
| Status | valid |
| Publication |
|
| Navigator | Notes |
LETTER of the Ministry of Health of the USSR dated 02.10.87 N 02-14 / 82-14 "ON THE PROCEDURE FOR EXPANDING INDEPENDENCE AND INCREASING THE RESPONSIBILITY OF THE HEADS OF HEALTH CARE AUTHORITIES WHEN APPLYING THE ORDER OF THE MINISTRY OF HEALTH OF THE USSR OF AUGUST 13, 1987 N 955"
Chapter 2
2.1. Working time budget for medical staff
One of the main indicators in the design of labor standards in all types of health care institutions, the analysis of the volume of work of a position is the working time budget.
Determination of the annual budget of working time of medical personnel has its own characteristics, in contrast to that adopted in the manufacturing sector. National economy.
When planning the number of workers in the main professions in the industrial sectors of the national economy, their attendance and payroll composition is taken into account and the methodology for calculating the number of employees is applied, that is, live work force to fulfill the planned plan, taking into account all the factors that prevent the employee from being at the workplace.
Labor rationing in health care has its own specifics and is methodically solved according to the job principle, according to which a certain amount of work is to be performed under certain conditions. organizational conditions one position, regardless of the number of persons who will perform work in this position during the year. This involves working a specific time during the working day and the number of working days in a year. In health care institutions, therefore, it is not the number of living labor forces that is determined, but the number of staff positions.
Under the medical position is understood the range of duties and the specific scope of work of a doctor on certain period working hours, regulated by the calculated norms of the doctor's workload, the duration of working hours and the duration of vacation. The position, as an indicator of the health plan, is a measure of the doctor's workload in various fields his activities.
The content of the concept of "medical position" to the concept of "doctor", as to an individual, corresponds only in the case when one doctor will perform work in one medical position and the balance of working time for this position will fully correspond to the actually worked working time by the doctor during the year in accordance with the established working hours under the current legislation.
However, during the year, doctors are absent from work due to illness, in connection with pre- and post-natal leave, caring for a child, sick family members. In addition, medical personnel are often distracted from work related to the provision of medical and preventive care to the population, to take advanced courses and specializations, work in various commissions and at meetings, and perform state and public duties. In these cases, the head of the institution during the absence of the employee has the right to invite another person as his deputy and thereby ensure the fulfillment of the planned scope of work. At the same time, an employee’s absence from work in a healthcare facility does not delay the work of other personnel, and the work itself can be performed on a different shift. At the same time, the absence in many cases of sufficient work to introduce full positions in a health care institution, it allows you to establish fractional parts of it and occupy it with part-time workers. Thus, the presence of part-time employment and substitution, which makes it possible to replace a doctor during his absence on vacation, due to illness and other valid reasons, actually predetermines the difference in labor rationing in healthcare from industrial sectors of the national economy.
The calculation of the planned duration of working hours during the year of medical personnel is carried out by excluding weekends and holidays, the duration of vacation from the number of calendar days in the year.
There are 365 calendar days in a year, including 52 days off and 8 holidays. Since one of the holidays in the year usually coincides with Sunday, 59 days off and holidays in the year are taken into account. The total duration of leave for health workers entitled to one or more types of additional leave is the sum of the main leave of 12 working days and the duration of the additional leave(s). According to the "List of industries, workshops, professions and positions with harmful working conditions, work in which gives the right to additional leave and reduced working hours" (section "Healthcare"), approved by the Decree of the State Committee of the Council of Ministers of the USSR on Labor and Wages and the Presidium of the All-Union Central Council of Trade Unions of October 25, 1974 N 298 / P-22, medical workers have an additional vacation of 6, 12, 18, 24 and 30 working days depending on the position held and place of work.In addition, some employees are provided with additional paid holidays in excess of those provided for in this resolution:
An additional paid three-day leave is provided to doctors of district hospitals and outpatient clinics located in countryside, district therapists and pediatricians of territorial city polyclinics, mobile teams of stations and emergency and emergency medical care stations, air ambulance stations and departments of planned and emergency advisory assistance for continuous work in these institutions and territorial areas for more than 3 years;
Additional leave is granted to donors after each day of blood donation; mothers with 2 or more children under the age of 12, if annual leave in total duration does not exceed 28 calendar days; students of higher and secondary specialized educational institutions for the period of performing laboratory work, passing tests and exams.
A necessary element in calculating the annual working time budget of a position is the number of hours worked per day.
For most doctors and nurses, a reduced working time is set - no more than 38.5 hours a week, due primarily to neuropsychic stress at work. Doctors and nurses, as a rule, are set a working day of 6.5 hours with six-day working week, for junior medical personnel - 7 hours On the eve of weekends and holidays, the working day is reduced by 30 minutes, and for workers with a 7-hour working day - by 1 hour. staff, a working day of 6 hours is established: in tuberculosis and infectious diseases hospitals and departments, psychiatric, neuropsychiatric, narcological and neurosurgical institutions and departments.In these cases, the working day is not reduced on weekends and holidays.For some medical workers, an even shorter working day is set ; so, 5.5 hour working day have, for example, doctors of medical labor expert commissions(VTEK) and medical advisory commissions, dentists (except for in-patient dental surgeons), dentists and prosthetists.
In addition to junior medical staff, the following have a 7-hour working day:
Chief physicians and their deputies;
Doctors and paramedical personnel of sanatoriums general type and rest houses;
Diet nurses of all medical institutions and paramedical personnel of dairy kitchens;
Dental technicians.
Based on the above data on the number of days the position works in a year and the daily working time, the annual budget of the position’s working time is calculated, expressed in hours or minutes.
As mentioned earlier, during the working day of a doctor, on average, about 30 minutes. time is spent on work not related to the reception of patients, the provision of medical and preventive care to them, and this time must be taken into account and excluded when calculating the annual budget of the working time of the position.
Thus, the calculation of the annual budget of the working time of the position (in hours) is carried out according to the formula:
B \u003d a x (c - c) - d
a - the number of working days of the position in a year;
c - daily working time;
c - time spent during the day, not related to treatment diagnostic work;
d - reduction of working hours on weekends and holidays (in hours).
When calculating the number of positions of endoscopists, nurses for physiotherapy, massage, centralized sterilization nurses, etc., an annual time budget is determined, taken into account in conventional units.
Many researchers, analyzing the activities of outpatient clinics, come to the conclusion that the actual annual workload of doctors is lower than planned, while the daily workload of a doctor is often higher than it is provided for by the standards. This should be attributed both to the insufficiently satisfactory organization of the work of doctors, and to the fact that the doctor actually works at the reception for a significantly smaller number of days and hours than is provided for by the planned calculations of the workload of the medical position.
The problem of studying the loss of working time of medical personnel and ways to reduce them is given Special attention, since the incomplete use of working days in a year leads to a decrease in the availability, volume and quality of medical care.
As mentioned above, the days when a medical worker is absent from work, with the exception of weekends, holidays and vacations, are not taken into account when calculating the planned budget of the position's working time, which is due to the system of substitution and part-time work in healthcare.
At the same time, in healthcare institutions, it is necessary to analyze the reasons for absenteeism, the possibilities of replacing an absent employee in accordance with the current legislation (Fig. 4).
Based on the materials of a specially conducted study of the level and structure of loss of working time of 765 doctors in 20 outpatient clinics, the number of days a doctor is absent from work during the year averages 41.7 days.
More than half of these losses are due to temporary disability due to illness, pre- and post-natal leave. Specialization and improvement, business trips, performance of state duties, account for about 20%, i.e. 9 days.
The full use by the head of the institution of the possibilities of substitution and part-time work in monitoring the working out of the corresponding working time will contribute to a more rational distribution of personnel and reduce the difference between the planned budget of the position's working time and the indicators of its actual use.
Rice. 4
ANNUAL BUDGET OF WORKING TIME OF MEDICAL STAFF
2.2. Regulation of the work of medical personnel of outpatient clinicsThe regulation of the work of medical personnel in outpatient clinics is based mainly on the study of the work of medical personnel. The design of standards for the positions of doctors conducting outpatient appointments is carried out according to two leading indicators:
1. The needs of the population in different types medical care, expressed in terms of attendance.
2. The planned function of a medical position.
The basis for determining the needs of the population in one form or another of medical care are the intensive indicators of attendance developed in scientific research for the prospective period, which reflect the nature of the pathology of the population, the incidence rate, the demographic situation, as well as the achievements medical science and the effect of their implementation in healthcare practice. Indicators of the population's need for outpatient care are established on the basis of a comprehensive methodology, including the study of morbidity by request, in-depth medical examinations of the population, the use of an expert assessment of the completeness and quality of medical care. However, the lack of distribution of attendance by types of institutions (service levels), the purpose of the visit create significant difficulties in their application in regulatory research work. In addition, the morbidity identified as a result of additional medical examinations taking into account the application of the expert method, as a rule, it is not implemented in the form of appeals from the population to healthcare institutions. The task of planning, of which labor rationing is an integral part, is the most rational combination of the real possibilities of health care institutions and the desire to satisfy the population's need for medical care to the maximum.
Determining the needs of the population in one form or another of medical care for the purposes of regulation is based on the study of three groups of data:
1. Materials of scientific research on the needs of the population in medical care.
2. Indicators of the activity of doctors of the studied types of institutions in 19 economic and geographical regions of the country, used as bases for collecting materials on labor.
3. Performance indicators of medical personnel in specially selected institutions, staffed, using advanced, progressive forms of service, methods of prevention, diagnosis and treatment.
As a rule, the difference in attendance rates between the second and third group of institutions is 15-20%. For example, the level of attendance of the population to phthisiatricians in city dispensaries for institutions of the second group was 168 per 1000 population, and the third group - 203.
To compare these data with the first group of indicators - the scientifically developed need of the population in one form or another of medical care - an appropriate analysis and refinement of the indicator is required.
This is due to the fact that in normative research studies the attendance of the population in a particular specialty in a particular type of institution is studied. The need is determined as a whole for the entire population at all stages of medical care. Recalculations of indicators taking into account the proportion of urban and rural residents, scientific research data on the distribution of attendance by stages of medical care provide a single summary indicator that reflects the population's need for a particular type of medical care. The implementation of meeting the needs of the population for the type of assistance being studied depends both on the degree of development of the service and on its accessibility.
It is legitimate to compare the actual indicators of attendance of the population with the data of need only in general for all specialties, taking into account the level of development of specialized services, since a possible "underload" in the number of visits in one specialty or another can be compensated to a certain extent by higher performance indicators in another, broader specialty. However, even such a comparison cannot claim to be a complete analysis, since it does not take into account the proportionality or possible disproportions in the development of outpatient, inpatient and emergency medical care.
A prospective indicator of the population's need for outpatient services is determined on the basis of data on the actual attendance of the population in the third group of institutions with a retrospective analysis of attendance rates for a number of previous years (3-5 or more). Then, the average increase in the number of visits per year is calculated as the arithmetic mean using the formula:
| a = | b - b_1 | (2.2.1.) | |
| n |
a - average annual increase in the number of visits to doctors;
b - the level of attendance to doctors of the given accounting year;
b_1 - the level of attendance to doctors of the base year compared with the reference year;
n - duration of the base period in years.
At the same time, the optimal value of the standard requirement for a promising five-year period is determined by the formula:
| H=b+5a | (2.2.2.) |
H is the predicted attendance by the end of the 5-year period.
In a number of cases, during the formation and development of a new medical specialty, an increase in the number of visits can occur exponentially, and the planning of the regulatory need for the near future is carried out by extrapolating the exponential growth in attendance:
| H = b x (I + | b_2 | ) | n | <*> | (2.2.3.) | |
| 100 |
b_2 - annual increase in the number of visits in %%;
n is the duration of the planned period in years.
<*>G.A. Popov, 1974
Thus, the value of the attendance indicator, taken as a starting point when designing the standard for the positions of doctors in outpatient clinics, is based on determining the level of attendance and analyzing its dynamics.
The function of a medical position is determined by the amount of work that must be performed within the annual balance of working time for this position.
A variety of factors influence the productivity of the outpatient doctor, that is, the indicator of his workload: the structure of visits by nosological forms, the nature and severity of the pathology, the ratio of primary and repeated visits, as well as visits made in connection with morbidity, with a preventive purpose , dispensary observation, etc.; the level of qualification of the doctor, his technical equipment, the availability of assistants, the organization of work, etc. (Fig. 5). The average time spent on the first visit is an integrating value that reflects the influence of various factors related both to the nature of the visit and the age and sex composition of patients, and to the forms and conditions of the organization of work of doctors. This involves the development of differentiated labor standards and the subsequent calculation on this basis of a single load, taking into account the diversity of activities of medical personnel.
The final data on labor costs obtained as a result of consolidation, expressed in time, allow us to calculate them in the "visit" indicator, the number of which per unit of working time (hour) determines the medical workload at an outpatient appointment (60 min: M min \u003d H).
Rice. 5
FACTORS CONSIDERED WHEN DESIGNING LABOR STANDARDS FOR OUTPATIENT INSTITUTIONS
In the future, the transition from indicators of labor costs to the indicator "position" is carried out. Currently, the indicator and measure of the volume of outpatient care in terms of health care is the "medical position".
The number of visits that a doctor's office must complete in a year is called the function of the doctor's office. It is expressed by the formula:
| F \u003d (A x t_a) + (B x t_b) + (C x t_s) x B | (2.2.4.) |
Ф - function of the medical position (number of visits);
A, B, C - doctor's workload for 1 hour of work in the clinic, during preventive examinations, providing assistance at home, respectively;
t_а, t_b, t_с - the number of hours of work per day for the given type of work;
The workload of a doctor at an appointment in a polyclinic and at home is regulated by the calculated service standards for doctors in outpatient clinics, approved by the USSR Ministry of Health or obtained as a result of scientific research. The annual balance of working time is determined based on the number of working days in a year and the length of the working day, in accordance with the current labor law. The beginning and end of work, the distribution of working time by type of activity during the accounting period is established by the shift (work) schedule approved by the administration in agreement with the trade union committee, depending on specific conditions. The work schedule of medical personnel can be very different not only in different health care institutions, but also among doctors of the same specialty of the same outpatient clinic. The distribution of a doctor's working time for outpatient appointments and care for patients at home should be differentiated taking into account the size and age composition of the population, the level of morbidity and seeking medical care, and the characteristics of the site.
Since the norms of service for 1 hour at the clinic, preventive examinations and the provision of medical care at home are not equivalent, the function of a medical position is different depending on the work schedule, with other equal conditions.
Example. If, on average, a district general practitioner during a working day spends 4 hours on an appointment at a polyclinic, of which 1 hour is for preventive examinations, and 2 hours for providing medical care at home, then
F = (5 x 3) + (7.5 x 1) + (2 x 2) x 282 = 7473 visits.
With a different work schedule, in the case when the general practitioner allocates 2.5 hours for an appointment at a polyclinic, 1 hour for preventive examinations and 2.5 hours for home care, the planned function of a medical position will be
F = (5 x 2.5) + (7.5 x 1) + (2 x 2.5) x 282 = 7050 visits.
When developing standards for outpatient medical positions, it is necessary to have a stable indicator of a planned medical position, standardized for all the specified parameters. Such requirements are met by converting all types of visits into units equivalent to any one of them, for example, visits to a polyclinic. The method of conversion to equivalent units is quite widely used in health economics.
The calculation of the total number of visits in equivalent units is carried out according to the formula:
| P \u003d A x 1 + B x K_1 + C x K_2 | (2.2.5.) |
P is the total number of visits in equivalent units;
A - the number of medical and diagnostic visits to the clinic;
B - number of preventive visits;
C is the number of home visits;
К_1,2 - coefficient of conversion of the corresponding visits into units equivalent to visits in the polyclinic.
With this calculation, the planned function of the position of a local general practitioner, regardless of the work schedule, will be 8460 visits (5 x 6 x 282).
It is also possible to eliminate the influence of a different work schedule of a doctor during the day, month, year on the value of the function of the position and, consequently, the indicator of the staffing standard using another methodological approach, calculating the weighted average number of visits per 1 hour of work using the formulas:
| P = | 100 | or | (2.2.6.) | ||||||
| m | + | n | + | p | |||||
| M | N | P | |||||||
| P = | 60 | (2.2.7.) | ||||||||||||||
| ( | 60 | ) | x m | ( | 60 | ) | x n | ( | 60 | ) | xp | |||||
| M | + | N | + | P | ||||||||||||
| 100 | 100 | 100 | ||||||||||||||
P - weighted average number of visits per 1 hour of work;
m, n, p - specific gravity the number of treatment and diagnostic, preventive visits and home visits in the overall structure of attendance in%%;
M, N, P - design load rate on different kinds visits.
The final stage in the development of a normative indicator is the transition from the measure of the volume of activity of the position in the number of visits to the measure "population", which is more convenient for practical application. The calculation of the standard is carried out according to the formula:
| H = | P x H | (2.2.8.) | |
| F |
N - the standard of a medical position;
P - attendance rate per 1 inhabitant per year;
P - the population for which the standard of a medical position is calculated (10 thousand, 100 thousand);
Ф - planned function of a medical position.
Calculation example. A scientific study found that the planned number of visits per 1 adult resident per year to a district general practitioner is 4.3, including 2.4 medical diagnostic, 1.2 preventive and 0.7 visits to provide medical care at home (table 5).
Table 5
Distribution of visits to the district general practitioner per 1 adult resident per year
| NN p/n | Type of visit | Number of visits | Structure of visits in %% | TO | Number of equivalent visits |
| 1 | 2 | 3 | 4 | 5 | 6 |
| 1. | Therapeutic-diagnostic | 2,4 | 55,8 | 1.0 | 2.4 |
| 2. | Preventive | 1,2 | 27,9 | 0,667 | 0,8 |
| 3. | at home | 0,7 | 16,3 | 2,5 | 1,75 |
| Total: | 4,3 | 100,0 | 4,95 |
1 calculation option (according to formula 2.2.5.). The function of the position of a local general practitioner in conditional outpatient medical and diagnostic visits is 8460 visits. The planned number of conditional equivalent visits is obtained by multiplying the number of various kinds of visits (column 3) by the value of the coefficient (column 5) and is 4.95 conditional visits taken into account, and then the value of the standard for the position of a district general practitioner is 5.9 positions in per 10,000 adults:
| H = | 4.95 x 10000 | = 5,9 |
| 8460 |
2 calculation option (according to formula 2.2.6). The weighted average number of visits per 1 hour of work of a district general practitioner with this structure of visits will be 4.342:
| P = | 100 | = 4,342 | |||||
| 55,8 | + | 27,9 | + | 16,3 | |||
| 5 | 7,5 | 2 | |||||
The same result is obtained when using formula 2.2.7 when calculating the weighted average load per 1 hour of work.
| P = | 60 | = 4,342 | |||||||||||
| ( | 60 | ) | x 55.8 | ( | 60 | x 27.9 | ( | 60 | x 16.3 | ||||
| 5 | + | 7,5 | + | 2 | |||||||||
| 100 | 100 | 100 | |||||||||||
From here, the function of the position of a general practitioner will be equal to 7347 visits per year (6 x 4.342 x 282) and the size of the staff standard - 5.9 positions of a district general practitioner per 10 thousand of the adult population:
| H = | 4.3 x 10000 | = 5,9 |
| 7347 |
The main task of hospitals of medical and preventive institutions is to ensure the full scope of examination and treatment of the patient in accordance with the material and personnel capabilities at different periods of his stay in the hospital (admission, examination, treatment, discharge) and at various stages of care (resuscitation and intensive care, active treatment, post-treatment and rehabilitation treatment) in conditions of continuity of the diagnostic and treatment process during the day.
The amount of time spent by medical personnel when servicing patients in a hospital is influenced by numerous factors, the main of which are: the composition of patients according to nosological forms of diseases; medical measures corresponding to the period of the patient's stay in the hospital, depending on the order of admission (scheduled or emergency hospitalization); average length of hospital stay (Fig. 6).
In addition, the degree of satisfaction of the needs of the population in hospital care, other things being equal, has an indirect impact on the standards for the work of medical personnel in hospitals.
The consolidation of the worker's load indicators depending on the indicated factors to obtain a single weighted average is carried out, as in the case of labor rationing in outpatient clinics, using a stepwise method.
Rice. 6
STANDARD FORMING FACTORS CONSIDERED IN THE DEVELOPMENT OF LABOR STANDARDS IN HOSPITAL INSTITUTIONS
In carrying out this work, the researcher uses a different sequence of calculations. For example, at the first stage, the labor costs for servicing patients with various nosological forms of diseases are determined, taking into account the age and sex composition of those hospitalized by periods of inpatient treatment.
Photochronometric observations, which are usually carried out within two weeks, do not always reveal the true workload of an employee for a number of work performed during the year, especially for rarely performed instrumental and hardware methods of examination. In this case, the data of photochronometric observations are supplemented by timing measurements. If it is impossible to implement them, data on time costs obtained from workers directly carrying out these manipulations and studies are used. The number of these studies during the year is set on the basis of the performance of the unit for calendar year, obtained from the "Map of the volume of activity of medical personnel of a healthcare institution" based on the data of accounting documentation.
So, for example, a urologist, according to photochronometric observations, spends 30 minutes on these types of activities, i.e. an average of 1.2 min. per treated patient. The volume of these studies is established from the "Map of the scope of activities ...", it is 0.8 examinations per patient, and, therefore, the estimated time spent per patient with an average length of stay in the hospital of 13 days will be 1.85 minutes.
Thus, comparison of data from direct observations with the annual volume of an employee's activity makes it possible to more objectively establish the costs of his labor for certain types of work.
Further calculation of the aggregated indicator is carried out according to the formula:
| M + K x M_l x (-2 - | n | ) + M_v | |||
| M = | 7 | (2.3.1.) | |||
| n- | n | ||||
| 7 |
M - weighted average time spent on direct patient care per one examination (in minutes);
M_n - the doctor's time spent on providing medical care to the admitted patient (in minutes);
M_l - the doctor's time spent on providing medical care to the patient on the day of the examination (in minutes);
M_v - the doctor's time spent on providing medical care to a discharged patient (in minutes);
K - coefficient of frequency of medical examinations of treated patients per doctor's working day;
N is the average duration of inpatient treatment (in days);
7 is the number of days in a week.
As a rule, a doctor examines a patient in a hospital daily, then K = I. In some cases, due to the specifics of medical work and the contingent served, the number of patient examinations per day deviates from one in one direction or another. So, in the departments (wards) of resuscitation and intensive care, in the maternity ward, during the working day, the doctor interviews and examines the patient several times. In psychiatric hospitals, sanatoriums, aftercare departments, a medical examination is possible once every 2, 3 or more days, in children's sanatoriums - once every 5 days, etc. Therefore, the inspection frequency coefficient is 0.5, respectively; 0.3 and 0.2.
This method calculates the doctor's costs directly related to patient care: interview, examination, medical care and documentation. In the future, the time during the working day spent on other types of work (auxiliary activities, official conversations, transitions, etc.) and personal time is determined.
When rationing the work of medical personnel, the work of the doctor in the evening and at night, on generally established weekends and holidays (the so-called "duty") is also taken into account. Medical care for patients at this time, as a rule, is provided by doctors, whose positions are provided for by staff standards for this institution, within their working hours for the accounting period. Physicians conducting medical work are involved in these works. Radiologists engaged exclusively in diagnostic work, laboratory assistants, and bacteriologists are not involved in "duty" duties. These physicians may be assigned to the so-called "duty" in their specialty.
"On duty", the duration of which, as a rule, should not exceed 12 hours, is carried out for the hospital as a whole, and in large hospitals, in addition, for a group of departments, if there are at least 200 beds in the group. Rural health facilities and maternity hospitals in cities may introduce "home calls".
The obtained data on the doctor's time spent on all types of work performed make it possible to calculate them in the "patient" indicator according to the formula:
| N_b | T - V - D | (2.3.2.) | |
| M |
Where H_b is a measure of the indicator "sick" (the doctor's workload per working day);
T - the duration of the working day for this position (in minutes);
B - the average time during the working day, not related to the direct service of patients (in minutes);
D - the average time excluded from the duration of the working day for the performance of "duty" (in minutes);
M - the average estimated time for servicing 1 patient (from formula 2.2.1.).
Calculation example.
The therapist spends an average of 15 minutes daily. for one patient. During the month, 24 hours are provided for "duty", i.e. daily working time is reduced by an average of 1 hour; the average time during the working day, not related to the direct service of patients, is 0.5 hours, therefore:
To move to the indicator adopted for calculating the staff of hospital institutions - "bed", the following methodological technique is used. It is known that the planned duration of a bed in a year is not the same in institutions of various types: for city hospitals it is 340 days, for rural hospitals - 320, for infectious diseases - 310, maternity hospitals - 300. Thus, during the year, part of the hospital beds are idle, since not occupied by patients for a number of reasons. Therefore, when moving from the "sick" indicator to the "bed" indicator, it is necessary, taking into account the planned duration of the bed occupancy in a year, to increase the previously obtained calculated indicator:
| N_k | 365 | x N_b | (2.3.3.) | ||||||
| P | |||||||||
| T = SUM(n_1 x t_1 + n_2 x t_2 +... + n_1 x t_1) | (2.4.1.) |
T - annual volume of activity, expressed in minutes or the number of conventional units;
n - number of studies, procedures;
t - in minutes or conventional units per study, procedure.
In cases where one structural unit the estimated norms of time are valid, expressed both in minutes and in conventional units, T is determined separately for these indicators.
The calculation of the required number of posts (W) to perform the annual volume of work is carried out according to the formula:
| W= | T | (2.4.2.) | |
| B |
T - corresponds to the formula 2.4.1;
B - the annual budget of the working time of the position.
The annual budget of working time for the positions of medical personnel of the auxiliary medical and diagnostic service can be expressed, as indicated in the relevant section, in minutes or in conventional units. Thus, the annual budget of a laboratory assistant, laboratory assistant, doctor and nurse for functional diagnostics is 101,910 minutes, a radiologist - 66,240 minutes, a physiotherapy nurse - 15,000 conditional physiotherapeutic units, a massage nurse - 8340 massage units.
As a rule, the indicator by which the standard for the position of medical personnel of an auxiliary medical and diagnostic service in outpatient and polyclinic institutions is determined is medical positions leading an outpatient appointment, and in hospital and sanatorium institutions - a bed.
The standard for the positions of medical personnel of the auxiliary medical and diagnostic service is calculated by the formula:
| N= | F | (2.4.3.) | |
| W |
N - position standard;
F - indicator of the standard (number of medical posts conducting outpatient appointments or number of beds);
W - corresponds to the formula 2.4.2.
Table 6
CALCULATION OF THE ANNUAL COST OF TIME OF THE LABORATORY MEDICAL STAFF FOR LABORATORY STUDIES
| Name of the study | Number of studies (n) | Time for 1 examination in min. (t) | Total Time (T) | ||
| for a laboratory assistant | for laboratory doctor | for a laboratory assistant | for laboratory doctor | ||
| Leukocyte count | 50000 | 2 | 6 | 50000 x 2= 100000 | 50000 x 6 = 300000 |
| Determination of the blood group | 1000 | 5 | 1000 x 5 = 5000 | ||
| Determination of amylase (diastase) in urine | 20000 | 15 | 20000 x 15 = 300000 | ||
| Examination of tumor punctures | 500 | 6 | 14 | 500 x 6= 3000 | 500 x 14 = 7000 |
| Total: | 100000 + 5000 300000 + 3000 = 435000 | 300000 + 7000 = 307000 | |||
An example of calculating the standard for the position of a laboratory assistant in an outpatient clinic
The volume of work indicated in the previous example, corresponding to 4,268 positions of laboratory assistants, is carried out in a polyclinic with 33.75 positions of outpatient doctors:
Those. the standard is set at the rate of 1 position of a laboratory assistant for 8 positions of doctors conducting outpatient appointments.
An example of calculating the standard for the position of a laboratory assistant in a hospital institution
The specified amount of work, corresponding to 4,268 positions of laboratory assistants, is carried out in a hospital with 210 beds.
| F x D x T x H |
N - position standard;
B - the annual budget of the working time of the position;
Ф - bed turnover;
D - the proportion of patients in need of research, procedures (in%%);
T - average estimated or standard time for 1 study, procedure, examination;
N - the number of procedures, studies, examinations for a course of treatment.
Formula 2.4.4. It is convenient because its components can be used to evaluate to a certain extent the organization of the diagnostic and treatment process, the completeness and quality of medical care for patients and make adjustments based on expert assessments. This formula is applicable mainly in scientific research.
Calculation example
In the hospital, the bed turnover is 20, of all patients, 30% need therapeutic massage, the number of standard massage units per procedure is 2.2 units; an average of 12 procedures are performed per course of treatment
| N= | 8340 x 100 | = 52.6 beds |
| 20 x 30 x 2.2 x 12 |
Those. the position of a massage nurse is established for 50 beds.
When changes are made to one of the indicators, the standard changes. So, if the selection of patients for treatment is determined not at 30, but at 60%, then the standard for the position will be 25 beds, with a decrease in the average number of procedures from 12 to 10-60 beds, etc.
In a number of cases, when rationing the work of paramedical personnel of an auxiliary medical and diagnostic service, a ratio standard is used. Thus, the number of positions of radiologists is set according to the number of positions of radiologists.
-
 Cash on delivery: what is it?
Cash on delivery: what is it?
-
 Law on LLC with the latest amendments Interest in the company's transaction
Law on LLC with the latest amendments Interest in the company's transaction
-
 Law on LLC with the latest changes What changes have been made
Law on LLC with the latest changes What changes have been made
-
 Opening IP: step by step instructions
Opening IP: step by step instructions
-
 Moon without a course in April. Moon without a course. Moon phenomena without a course
Moon without a course in April. Moon without a course. Moon phenomena without a course
-
 What professions are now in demand and highly paid?
What professions are now in demand and highly paid?
-
 Notification of the commencement of entrepreneurial activity: why and where to submit a notice of the commencement of entrepreneurial activity to Rospotrebnadzor
Notification of the commencement of entrepreneurial activity: why and where to submit a notice of the commencement of entrepreneurial activity to Rospotrebnadzor
-
 Electronic library systems Electronic library system of yurayt publishing house
Electronic library systems Electronic library system of yurayt publishing house
-
 Employment contract for micro-enterprises Employment contract template approved by the government of the Russian Federation
Employment contract for micro-enterprises Employment contract template approved by the government of the Russian Federation



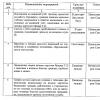

2023
newmagazineroom.ru - Accounting statements. UNVD. Salary and personnel. Currency operations. Payment of taxes. VAT. Insurance premiums