This job description has been translated automatically. Please note that automatic translation does not provide 100% accuracy, so there may be minor translation errors in the text.
| Instructions for the position " Occupational Therapy Instructor", presented on the website, complies with the requirements of the document - "DIRECTORY of qualification characteristics of workers' professions. Issue 78. Healthcare. (As amended in accordance with the orders of the Ministry of Health N 131-O dated June 18, 2003 N 277 dated May 25, 2007 N 153 dated March 21, 2011 N 121 dated February 14, 2012)", which is approved Order of the Ministry of Health of Ukraine dated March 29, 2002 N 117. Approved by the Ministry of Labor and Social Policy of Ukraine. The status of the document is "valid". |
|
Preface to job description
0.1. The document comes into force from the moment of its approval.
0.2. Document developer: _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _.
0.3. Document approved: _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _.
0.4. Periodic verification of this document is carried out at intervals not exceeding 3 years.
1. General Provisions
1.1. The position "Instructor in occupational therapy" belongs to the category "Specialists".
1.2. Qualification requirements - incomplete higher education (junior specialist) in the direction of preparation "Medicine" for any specialty of a medical profile. Job specialization. No work experience requirements.
1.3. Knows and applies:
- current legislation on health protection and regulations governing the activities of healthcare institutions;
- organization of occupational therapy, principles and methods of its implementation in various diseases and significance for the rehabilitation of patients;
- Fundamentals of law in medicine;
- rights, duties and responsibilities of an occupational therapy instructor;
- basics of normal and pathological anatomy and physiology;
- labor protection rules for various methods of occupational therapy;
- rules for the provision of first and emergency medical care;
- Rules for the preparation of medical documentation.
1.4. An occupational therapy instructor is appointed to the position and dismissed by order of the organization (enterprise / institution).
1.5. The occupational therapy instructor reports directly to _ _ _ _ _ _ _ _ _ _ .
1.6. The occupational therapy instructor directs the work of _ _ _ _ _ _ _ _ _ _ .
1.7. The occupational therapy instructor during his absence is replaced by a duly appointed person who acquires the appropriate rights and is responsible for the proper performance of the duties assigned to him.
2. Description of work, tasks and job responsibilities
2.1. It is guided by the current legislation of Ukraine on health protection and regulatory legal acts that determine the activities of healthcare and social security institutions, the organization of medical care, including rehabilitation care for patients.
2.2. He uses modern methods of occupational therapy according to the prescriptions of doctors, works under their supervision.
2.3. Prepares premises and workplaces.
2.4. Provides the process of occupational therapy with raw materials, materials, tools, necessary equipment.
2.5. Determines with the doctor for each patient the methods and methods of labor, the transition from simple to more complex labor processes.
2.6. Supervises the fulfillment by patients of prescriptions for occupational therapy.
2.7. Provides labor protection.
2.8. He knows resuscitation techniques, is able to provide assistance in case of traumatic injury, bleeding, collapse, poisoning, drowning, mechanical asphyxia, anaphylactic shock, burns, frostbite, allergic conditions.
2.9. Adheres to the principles of medical deontology.
2.10. Maintains medical records.
2.11. Constantly improves his professional level.
2.12. Knows, understands and applies the current regulatory documents relating to its activities.
2.13. Knows and fulfills the requirements of regulatory acts on labor and environmental protection, complies with the norms, methods and techniques for the safe performance of work.
3. Rights
3.1. The Occupational Therapy Instructor has the authority to take action to prevent and remedy any irregularities or nonconformities.
3.2. An occupational therapy instructor has the right to receive all social guarantees provided for by law.
3.3. An occupational therapy instructor has the right to demand assistance in the performance of his duties and the exercise of his rights.
3.4. The occupational therapy instructor has the right to demand the creation of organizational and technical conditions necessary for the performance of official duties and the provision of the necessary equipment and inventory.
3.5. The occupational therapy instructor has the right to get acquainted with the draft documents relating to his activities.
3.6. The occupational therapy instructor has the right to request and receive documents, materials and information necessary for the performance of his duties and instructions from the management.
3.7. An occupational therapy instructor has the right to improve his professional qualifications.
3.8. The occupational therapy instructor has the right to report all violations and inconsistencies identified in the course of his activities and make proposals for their elimination.
3.9. The occupational therapy instructor has the right to get acquainted with the documents that define the rights and obligations of the position held, the criteria for assessing the quality of the performance of official duties.
4. Responsibility
4.1. The occupational therapy instructor is responsible for non-fulfillment or untimely fulfillment of the duties assigned by this job description and (or) non-use of the rights granted.
4.2. The occupational therapy instructor is responsible for non-compliance with the internal labor regulations, labor protection, safety, industrial sanitation and fire protection.
4.3. The occupational therapy instructor is responsible for disclosing information about the organization (enterprise/institution) that is a trade secret.
4.4. The occupational therapy instructor is responsible for non-fulfillment or improper fulfillment of the requirements of the internal regulatory documents of the organization (enterprise / institution) and the lawful orders of the management.
4.5. An occupational therapy instructor is liable for offenses committed in the course of his activity, within the limits established by the current administrative, criminal and civil legislation.
4.6. The occupational therapy instructor is responsible for causing material damage to the organization (enterprise/institution) within the limits established by the current administrative, criminal and civil legislation.
4.7. The Occupational Therapy Instructor is responsible for the misuse of the granted official authority, as well as the use of them for personal gain.
APPROVE:
[Job title]
_______________________________
_______________________________
[Name of company]
_______________________________
_______________________/[FULL NAME.]/
"______" _______________ 20___
JOB DESCRIPTION
Occupational Therapy Instructor
1. General Provisions
1.1. This job description defines and regulates the powers, functional and job duties, rights and responsibilities of an occupational therapy instructor [Name of the organization in the genitive case] (hereinafter referred to as the Medical Organization).
1.2. An occupational therapy instructor is appointed and dismissed in accordance with the procedure established by the current labor legislation by order of the head of the Medical Organization.
1.3. The occupational therapy instructor belongs to the category of specialists and is subordinate to [name of the position of subordinates in the dative case].
1.4. The Occupational Therapy Instructor reports directly to [title of immediate supervisor in the dative case] of the Medical Organization.
1.5. A person who has a secondary vocational education in the profile of the work performed or a secondary vocational (medical) education without presenting requirements for work experience is appointed to the position of an occupational therapy instructor.
1.6. The Occupational Therapy Instructor is responsible for:
- effective performance of the work entrusted to him;
- compliance with the requirements of performance, labor and technological discipline;
- the safety of the documents (information) that are in his custody (become known to him), containing (constituting) the trade secret of the Medical Organization.
1.7. The occupational therapy instructor should know:
- laws and other regulatory legal acts of the Russian Federation in the field of healthcare;
- fundamentals of physiology and pathophysiology of the body;
- the basics of occupational therapy and its role in the medical rehabilitation of patients;
- organization of work on occupational therapy;
- principles of selection of rational methods of work;
- medical ethics;
- psychology of professional communication;
- fundamentals of labor legislation;
- internal labor regulations;
- rules on labor protection and fire safety.
1.8. The occupational therapy instructor in his work is guided by:
- local acts and organizational and administrative documents of the Medical Organization;
- internal labor regulations;
- rules of labor protection and safety, ensuring industrial sanitation and fire protection;
- instructions, orders, decisions and instructions of the immediate supervisor;
- this job description.
1.9. During the temporary absence of an occupational therapy instructor, his/her duties shall be assigned to [deputy position].
2. Job responsibilities
The occupational therapy instructor performs the following labor functions:
2.1. Carries out work with patients on occupational therapy in accordance with doctor's prescriptions, transferring them from simple to more complex labor processes.
2.2. Prepares a workplace for the patient and provides it with raw materials, materials, tools and equipment.
2.3. Monitors the safe working conditions of patients and their performance of labor functions.
2.4. Keeps a daily record of the consumption of raw materials and materials by patients, the use of tools and the storage of leftover raw materials, materials and finished products in accordance with established forms.
In the event of a business need, an occupational therapy instructor may be involved in the performance of his duties overtime, in the manner prescribed by the provisions of federal labor law.
3. Rights
The occupational therapy instructor has the right to:
3.1. Give subordinate employees and services instructions, tasks on a range of issues included in functional duties.
3.2. Control the execution of production tasks, the timely execution of individual orders and tasks by subordinate services.
3.3. Request and receive the necessary materials and documents related to the activities of an occupational therapy instructor, subordinate services and divisions.
3.4. Interact with other enterprises, organizations and institutions on production and other issues related to the competence of an occupational therapy instructor.
3.5. Sign and endorse documents within their competence.
3.6. Submit for consideration by the head of the Medical Organization submissions on the appointment, transfer and dismissal of employees of subordinate units; proposals for their promotion or for the imposition of penalties on them.
3.7. Enjoy other rights established by the Labor Code of the Russian Federation and other legislative acts of the Russian Federation.
4. Responsibility and performance evaluation
4.1. An occupational therapy instructor bears administrative, disciplinary and material (and in some cases, provided for by the legislation of the Russian Federation, also criminal) responsibility for:
4.1.1. Non-fulfillment or improper fulfillment of official instructions of the immediate supervisor.
4.1.2. Failure to perform or improper performance of their labor functions and assigned tasks.
4.1.3. Unlawful use of the granted official powers, as well as their use for personal purposes.
4.1.4. Inaccurate information about the status of the work entrusted to him.
4.1.5. Failure to take measures to suppress the identified violations of safety regulations, fire and other rules that pose a threat to the activities of the enterprise and its employees.
4.1.6. Failure to enforce labor discipline.
4.2. Evaluation of the work of an occupational therapy instructor is carried out:
4.2.1. The immediate supervisor - regularly, in the course of the daily implementation by the employee of his labor functions.
4.2.2. Attestation Commission of the enterprise - periodically, but at least once every two years based on the documented results of the work for the evaluation period.
4.3. The main criterion for evaluating the work of an occupational therapy instructor is the quality, completeness and timeliness of his performance of the tasks provided for in this instruction.
5. Working conditions
5.1. The work schedule of an occupational therapy instructor is determined in accordance with the internal labor regulations established by the Medical Organization.
6. Right to sign
6.1. In order to ensure his activities, the occupational therapy instructor is granted the right to sign organizational and administrative documents on issues referred to his competence by this job description.
Familiarized with the instruction ___________ / ____________ / "____" _______ 20__
font size
ORDER of the Ministry of Health and Social Development of the Russian Federation dated 06-11-2009 869 (as amended on 03-03-2010) ON APPROVAL OF THE UNIFIED QUALIFICATION DIRECTORY ... Relevant in 2018
Occupational Therapy Instructor
Job responsibilities. Carries out work with patients on occupational therapy in accordance with doctor's prescriptions, transferring them from simple to more complex labor processes. Prepares a workplace for the patient and provides it with raw materials, materials, tools and equipment. Monitors the safe working conditions of patients and their performance of labor functions. Keeps a daily record of the consumption of raw materials and materials by patients, the use of tools and the storage of leftover raw materials, materials and finished products in accordance with established forms.
Must know: laws and other regulatory legal acts of the Russian Federation in force in the field of healthcare; fundamentals of physiology and pathophysiology of the body; the basics of occupational therapy and its role in the medical rehabilitation of patients; organization of work on occupational therapy; principles of selection of rational methods of work; medical ethics; psychology of professional communication; fundamentals of labor legislation; internal labor regulations; rules on labor protection and fire safety.
Qualification requirements. Secondary vocational education in the profile of the work performed or secondary vocational (medical) education without presenting requirements for work experience.
We bring to your attention a typical example of a job description for an occupational therapy instructor, sample 2019/2020. should include the following sections: general position, duties of an occupational therapy instructor, rights of an occupational therapy instructor, responsibilities of an occupational therapy instructor.
Occupational Therapy Instructor Job Description belongs to the section Qualification characteristics of positions of workers in the field of healthcare".
The occupational therapy instructor job description should include the following:
Job Responsibilities of an Occupational Therapy Instructor
1) Job responsibilities. Carries out work with patients on occupational therapy in accordance with doctor's prescriptions, transferring them from simple to more complex labor processes. Prepares a workplace for the patient and provides it with raw materials, materials, tools and equipment. Monitors the safe working conditions of patients and their performance of labor functions. Keeps a daily record of the consumption of raw materials and materials by patients, the use of tools and the storage of leftover raw materials, materials and finished products in accordance with established forms.
Occupational Therapy Instructor Must Know
2) An occupational therapy instructor, in the performance of his duties, must know: laws and other regulatory legal acts of the Russian Federation in the field of healthcare; fundamentals of physiology and pathophysiology of the organism; the basics of occupational therapy and its role in the medical rehabilitation of patients; organization of work on occupational therapy; principles of selection of rational methods of work; medical ethics; psychology of professional communication; fundamentals of labor legislation; internal labor regulations; rules on labor protection and fire safety.
Occupational Therapy Instructor Qualification Requirements
3) Qualification requirements. Secondary vocational education in the profile of the work performed or secondary vocational (medical) education without presenting requirements for work experience.
Occupational therapy instructor job description - sample 2019/2020. Occupational Therapy Instructor Job Responsibilities, Occupational Therapy Instructor Rights, Occupational Therapy Instructor Responsibilities.
State Institution "Center for Social Services for the Population of the City of Volsk"
Organizational and methodological department
Information material for employees of the social rehabilitation department

2010
In old age, a person tends to limit motor activity, mental activity decreases. One of the types of active leisure is occupational therapy. Occupational therapy helps older people to organize productively and enjoy an independent life. The main factor motivating older people to participate in occupational therapy is a sense of the importance of work, a sense of their own need. Occupational therapy is an active method of restoring and compensating impaired functions through various work aimed at creating a useful product. The general foundations of the physiological understanding of the therapeutic effects of labor are stated in the statements: “In labor, the strength of nervous processes is trained, their healthy correlation is formed and restored, the correct interaction of various systems in the brain, which is the basis of a healthy personality, the integrity of our “I”.
In occupational therapy, the very process of functioning of the lesions of the system acts as a healing, restorative and supporting factor. Labor movements and operations stimulate physiological processes, cause the harmonious functioning of the patient's main systems, mobilize his will, discipline, accustom to concentration of attention, create a cheerful mood, free (distract) from thoughts about the disease, excite psychological activity, directing it into the mainstream of a substantive, meaningful productive and satisfying activity.
When prescribing occupational therapy, the following rules should be followed:
1. Indications and contraindications for occupational therapy are determined by an individual assessment of the physical and mental state of the resident and the degree of functional damage.
2. The appointment of occupational therapy is carried out by a doctor. It determines the beginning of occupational therapy and the nature of the features (labor regimen, dosage, type of labor movements).
3. Occupational therapy is included in the system of a unified treatment and rehabilitation program and should be organically combined with other methods of treatment and rehabilitation used.
4. Preferably an earlier start, easy and affordable, appropriate to the possibilities of the resident occupational therapy.
5. Leading in its appointment are medical indications, but the effect of it is much greater when the personality characteristics and wishes of the patient are additionally taken into account.
6. Throughout the entire period of occupational therapy, medical monitoring and evaluation of effectiveness is necessary for the timely correction of labor operations, dosages and to achieve the maximum effect.
Absolute contraindications for occupational therapy
1. The general serious condition of the patient
2. Acute febrile conditions with a temperature above 38 degrees.
3. Tendency to bleed.
4. Causalgia.
Load Dosing in Occupational Therapy
The dosage of the load during occupational therapy is determined by the general condition of the resident, the localization of the pathological process, the volume of functional disorders, and the period of rehabilitation treatment.
Occupational therapy is dosed according to the labor regime, the type of labor movements and operations (observing the sequential transition from simple to more complex ones), the duration of classes, the frequency of their repetition during the day, week.
Distinguish between individual and group occupational therapy. With older citizens, it is recommended to conduct classes according to a group method, which allows you to restore impaired communication skills, smooth out the feeling of loneliness.
In the social and rehabilitation department, it is recommended to carry out the following types of occupational therapy:
1. Functional or restorative occupational therapy. This type is used for movement disorders. This type of occupational therapy should not be started from the moment of admission to the department, in view of the fact that some, at least an elementary restoration of the function of the corresponding organ is necessary.
There are three groups of labor operations: occupational therapy in a light mode (winding threads, making gauze bandages); occupational therapy, which develops (develops) strength, endurance of the muscles of the hands (sculpting, work with a planer, file, etc.); occupational therapy, developing fine coordination of finger movements, increasing their sensitivity (knitting, weaving, printing, etc.).
The selection of labor operations is an essential task of restorative occupational therapy. There are almost no labor operations that would require only unidirectional movements in some joint: where flexion and extension movements are required.
Despite the complex nature of each labor operation, there are very noticeable signs of similarities and differences between them. For example, almost all manual work involves the shoulder, forearm, hand, fingers, and various muscle groups are involved. However, in some, finger movements predominate, in others - movements in the elbow joint; some require a greater range of motion, others less; some refer to power movements, others to speed and precision. It is recommended to use the following types of feasible work: planting, transplanting, caring for indoor plants, planting seedlings, planting in the ground, caring for vegetables and fruit crops, planting flowers in flower beds on the site and caring for them; participation in subbotniks in the adjacent territory.
2. Recreational occupational therapy (occupational therapy.)
A person is characterized not only by obligatory, useful activity, but also by one in which he realizes individual interests and inclinations. This work is carried out by free choice and is not mandatory. It can have a variety of forms, be both entertaining and educational in nature, organized in the form of circles of interest. It is recommended to use needlework classes: knitting, embroidery, appliqué, repair of clothes and bed linen, etc. Board game lovers should be involved in playing chess, checkers, lotto, dominoes. Employment therapy helps patients to distract from thoughts about their disease, stimulates their communication, promotes mutual understanding, and helps to improve mood.
3. Self-care training (domestic rehabilitation).
Household rehabilitation is a system of teaching self-service to patients with impaired elementary motor functions of the limbs. More often, such disorders occur as a result of strokes, injuries, diseases of the musculoskeletal system. It is recommended to start household rehabilitation classes as early as possible, since its main goal is to eliminate the patient's helplessness. To train self-service skills, for citizens with limited mobility and self-service, it is recommended to use special devices (mobile tables, arcs, household items, various devices for performing movements with a brush, fingers). When clients become more mobile, self-service skills can be trained in the classroom and use items that a person uses at home: sets of tableware (plates, spoons, forks, knives, glasses, teapots, pots, pans, etc.); household items (gloves, buttons, zippers, belts, needles, brushes, telephone, alarm clock); household items (designer, abacus, plasticine); personal hygiene items (comb, toothbrush, soap, towel). At the next stage, it is recommended to involve residents in household rehabilitation to work in the department: making beds, participating in the distribution of food, performing morning and evening toilet. Self-service training may include imitation of everyday scenes: getting ready and going to the store, washing clothes, etc. Domestic rehabilitation should be carried out under the supervision of a nurse, an occupational therapy instructor.
For practical application, a convenient scheme for conducting household rehabilitation with consistent training of residents in various actions differentiated by complexity in the field of self-service:
Personal hygiene:
washing,
Teeth cleaning,
Shaving,
Combing.
Nutrition:
spoon food,
Eating with a fork, using a knife,
Drinking from a glass, cup.
Mastering clothes:
put on underwear,
Put on outerwear
fasten buttons,
lace up shoes,
Tie a Tie.
Mastering other hand movements:
Write the address, sign
Unlock and lock the doors
Open and close the window
Ring the doorbell,
Make a phone call,
Turn the lights on and off
Open and close the water tap,
Light a match.
Movement:
Walking on a flat surface
Climbing and descending stairs;
Overcoming obstacles (sand, gravel, groove),
Boarding a vehicle.
Training sessions
Training sessions are held with the elderly with disabilities intellectual-mnestic functions, speech defects.
The deterioration of intellectual-mnestic functions reflects a decrease in mental activity due to the weakening of the main processes of mental activity (excitatory and inhibitory). Recently, ideas about the intelligence of an elderly person have changed. The impression of a regular increase in the inferiority of the psyche of the elderly is untenable. More often, a decrease in intelligence is observed in those old people in whom it was limited from youth, and at an initially high level, it decreases more slowly. Moreover, the range of knowledge, practical acumen, ability to find solutions can grow. Difficulties in learning new things are compensated by the ability of associative thinking and the use of life experience. All this should be taken into account when using teaching methods for the elderly. This work should involve a psychologist, occupational therapy instructor, nurses, head of the department.
Training is possible according to two (formal and informal) methods.
Formal technique - includes teaching (school style) and is conducted in an isolated, equipped classroom. The training is carried out in a friendly, respectful atmosphere with the obligatory encouragement of correctly completed tasks, with repetition and successive complication of them, as they are mastered and adapted.
Informal work methodology with residents is a continuous process throughout almost his entire life, which involves both all the people around the elderly person (relatives, friends, acquaintances, social workers and nurses), and the things around him as sources of certain information.
It involves constantly reminding the patient "who is he?" (his name, patronymic, surname, age), where he is (at home, with friends, on the street, in the hospital, etc.), what is happening at the moment, who surrounds him (their belonging to him, names). In rooms it is necessary to have clocks, calendars with a mark of the current date; on the doors of rooms, wards, understandable, accessible and noticeable signs of the direction of movement of the patient, information stands and tables located at eye level, and a daily routine for the department are installed. Residents are given or read daily newspapers or other media.
Art therapy
Art therapy - active corrective influence through various forms of art; first of all - on the emotional status of patients. The method is used both independently and in the complex of a rehabilitation program. Art therapy goes well with music therapy, aromatherapy.
The specific tasks of art therapy work with the elderly are to overcome social isolation, increase self-esteem, create conditions for updating life experience, recognizing its values, and realizing one's creative potential.
Art therapy classes help to establish contact between the staff and the patient, since it is sometimes easier for him to express his emotional state on paper, and facilitate mutual understanding in various forms of aphasia.
There are two teaching methods:
1. Passive- the lesson is conducted by a teacher (psychologist, occupational therapy instructor, nurse, head of the department), and the residents listen and watch.
2. Active- the clients themselves actively participate in discussions, perform art therapy tasks, suggest topics.
When choosing forms of art therapy, one should take into account possible defects in hearing, vision, and impaired motor functions. Usually classes are held in the daytime 1-2 times a week, lasting 30-60 minutes in groups of 3-8 people. The vast majority of clients note an improvement in their emotional state and mood after art therapy, a decrease in irritability, a surge of vigor and vitality, creative activity appears, a desire to do something, and interpersonal contacts improve.
volunteer movement
Volunteer movement - voluntary assistance and participation of patients in some areas of work of the occupational therapy room, primarily occupational therapy and art therapy. Such joint work of patients and medical staff helps, on the one hand, to better establish interpersonal contacts and more fully understand the problems of the elderly; on the other hand, it makes it possible to realize experience and knowledge, which become less and less in demand with age.
PRIVATE METHODS OF OCCUPATIONAL THERAPY
Occupational therapy for movement disorders
In violation of motor functions, functional or restorative occupational therapy is used. The purpose of which is to influence the damaged part of the body, organ or system to restore the function disturbed by the pathological process through appropriately selected types of labor activity.
The movements of labor activity are familiar, habitual and natural. The patient's attention is focused on the result of the work, which distracts him from stiffness. However, a number of labor operations may be overwhelming (from functional positions). This forces the patient to find a workaround for the gradual involvement of the damaged organ in the work, which is more often manifested by a tendency to spare the affected organ or replace it with a healthy one. As a result, negative compensation occurs, in which the defect is not only not overcome, but is even more fixed (for example, the replacement of pronation and supination of the hand by rotation of the shoulder). From the point of view of restoration of function - negative compensation is harmful. There is a need to gradually accustom the diseased organ to movements that are temporarily inaccessible to it, which is ensured by determining the dosage and sequence of work.
According to (1946) there are six phases of the recovery process when using occupational therapy:
1 phase. The diseased limb is excluded from the labor process.
2 phase.The diseased limb begins to take part in the process as a support for the workpiece or tool (the diseased limb rests or lies). The transition to phase 3 is responsible, as a delay in phase 2 can make it difficult to deal with developing contractures or stiffness.
3 phase.A sick limb paired with a healthy one - the dynamic nature of the work. A healthy limb acts as a tractor. This phase is optional for all patients, there may be a transition from the second to the fourth, or it is possible to use labor operations from the 3rd phase. In addition, it is short lived. Patients with sharply reduced muscle tone may be delayed on it.
4 phase.It can be conditionally called the phase of removal of secondary defects. If, for example, a patient with damage to the elbow or wrist joint develops shoulder stiffness, then active movements begin in the shoulder joint. This phase can last from several days to several months.
5 phase.Shifts begin directly in the zone of the affected area, where there is already a gradual removal of primary defects. The diseased limb becomes a more or less complete organ. At the same time, patients often resort to compensatory methods. From this point of view, the 5th phase is the most responsible. Therapeutic tactics is as follows: with persistent defects (ankylosis, cicatricial contractures), it is necessary to adapt patients to work, allowing any compensation (for example, due to a healthy arm, unnecessary movements of the lower extremities and body, preserved muscles and joints of the diseased limb). restored, then you need to deal with various forms of negative compensation. In some cases, the recovery processes, after the removal of secondary defects, seem to stop and do not give any shifts in the primary defects. In such cases, it is recommended to load the affected area. The duration of phase 5 is highly variable.
6 phase.This is the final step of the fifth. It achieves a complete or almost complete restoration of the affected function. The diseased limb becomes a full-fledged working organ and does not need replacement techniques. This phase may not be relevant. Most likely, the 6th phase is reached by patients with minor motor disorders or those in whom secondary defects are quickly eliminated.
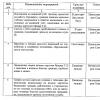
Method of functional tests.
Table 1.
The instructor explains to the resident the purpose and arrangement of the tools, demonstrates working methods. Further offers to do the same to the client.
movements | Functional working trials |
Abduction and adduction in the shoulder joint | Working with a rip saw |
Flexion and extension at the shoulder and elbow joints. Pronation and supination of the forearm | Work with a cross saw, hacksaw, file, planer. Work with a round file, and a screwdriver, centering |
Flexion and extension of the hand | Work with an ax, hammer, mallet |
Flexion and extension of the fingers in the metacarpal and interphalangeal joints | Work with pliers, pliers, scissors |
It is known that any labor operation can be performed not in one, but in several ways. The preference of one method to another is most often due to the patient's tendency to turn off movements that are difficult for him and replace them with those available to him - with switching to the work of intact muscles. For example, in the planing operation, patients often replace flexion-extension movements in the elbow joint with movements in the hip joint, as well as in the knee joint. Almost invariably, where agonists act, antagonists also act. This fact becomes absolutely clear if we remember that most of the labor movements are rhythmic in nature, with the alternation of oppositely directed movements inherent in the working rhythm: up-down, forward-backward, right-left, inside-out, etc.
Taking into account the clinic of the disease, the existing functional changes, the type of occupational therapy is also selected. Rehabilitation of the lost motor function is carried out in two ways: through the development of lost motor functions and adaptation (adaptation) of the patient to work.
The occupational therapy program can be conditionally divided into three stages: 1) diverting the patient from pain by minimally loading the affected limb and actively engaging the healthy limb in the work; 2) development of passive movements in the diseased limb; 3) development of active movements in the diseased limb.
Preparatory period: 1 - preparation of the workplace and materials for work (10-15 minutes); 2 - briefing (up to 10 minutes).
Main period: implementation of the main part of the planned work (20-60 minutes).
Final period: summing up the results of work - delivery of products, inventory, cleaning of the workplace (10-15 minutes).
A feature of occupational therapy classes is the mandatory introductory exercises before work and exercises that accelerate the rest of working muscles. With severe damage to the muscles and joints, the preparation of the neuromuscular apparatus to perform the specified movements can take 60-70% of the time of the entire lesson.
Basic Movement Disorder Terms:
Paralysis (plegia) - complete absence of muscle contraction.
Paresis - partial loss of motor function. Paralysis (paresis) of one limb is called monoplegia (monoparesis), two limbs of the same name are called paraplegia (paraparesis), two limbs of one side of the body are called hemiplegia (hemiparesis), three limbs are called triplegia (triparesis), four - tetraplegia (tetraparesis).
contractures - complete lack of movement in the joint.
Hyperkinesis - altered movements, devoid of physiological significance, arising involuntarily. These include convulsions, athetosis, trembling.
Сvroads - clonic are rapidly alternating muscle contractions and relaxations, tonic - prolonged muscle contraction.
Athetosis - slow worm-like movements of the fingers of the hand, torso, as a result of which it twists in a corkscrew-like manner when walking.
D birth (tremor) - involuntary rhythmic vibrations of the limbs and head.
Ataxia - violation of coordination, disproportion of motor acts (dynamic) and balance when standing (static).
Paralysis and paresis are of two types: spastic and flaccid.
Spastic paralysis is characterized by the absence of only voluntary movements, an increase in muscle tone and all tendon reflexes. An important element of the methodology is the education of the simplest motor skills of self-service (buttoning and unbuttoning buttons, dressing, picking up matches). For this purpose, exercises with small movements and modeling are given for the fingers.
Flaccid paralysis is manifested by the absence of both voluntary and involuntary movements, low tone and muscle atrophy, i.e., deeper functional disorders of the motor apparatus. So with lower flaccid paraplegia, the patient cannot move independently and he has to be on bed rest. The possibility of movement is associated with the use of crutches. With an increase in motor function, the necessary household skills are mastered: turn on the light, handle kitchen utensils, household items. Training of the supporting function of the legs, includes sewing on a sewing machine, carpentry and locksmith work, grinders and weaving machines with a foot drive.
In the process of training to master everyday skills in a patient, such coordination of movements gradually develops. In specially equipped rooms with a set of household appliances, stands on which they are mounted and strengthened, patients develop self-service skills.
For patients with impaired elementary functions of the limbs, self-service training is included in the occupational therapy system.
Labor tasks are selected in accordance with the nature of motor disorders, functional biomechanical features of the motor apparatus on the basis. Recovery is not immediate. The diseased organ should be loaded with active movements gradually, depending on the stage of the pathological process, the severity of complications, etc. There may be difficulties along the way that make it necessary to change tactics in choosing an operation and the duration of their use.
To restore the function of movement of the upper limbs, in particular the hand, it is possible to apply - weaving, knitting, carpentry and metalwork (table 2), sewing (table 3). So carpentry restores movement in the shoulder, elbow and wrist joints with the simultaneous participation of the shoulder girdle. For example, planing with a planer is associated with abduction and adduction of the scapula, flexion and extension of the shoulder and forearm. Working with a file allows you to involve the sick hand in the work with the help of a healthy one. Pronation and supination of the forearm is best restored with a screwdriver.
Variants of the nature of movements in carpentry and locksmith work.
Table 2.
Types of jobs | Movements performed | Working muscles |
Sawing (both hands) | Grasping the handle with fingers, flexion and extension in the elbow and shoulder joints | Finger flexion, biceps brachii, brachialis, triceps brachii, pectoralis major, coracobrachialis, latissimus dorsi, anterior and posterior deltoids |
Planing (both hands) | Grasping the handle, abducting 1 finger, flexion and extension in the elbow and shoulder joints with an emphasis on extension | The same muscles, abductor 1 finger of the right hand |
Sanding products (both hands) | Flexion and extension in the elbow and shoulder joints of the back | Biceps brachii, brachialis, triceps brachii, deltoid, pectoralis major, latissimus dorsi |
File work (both hands) | Flexion of the fingers of the right hand, flexion in the elbow joints (with effort), small movements in the shoulder joints | Flexors of the fingers of the right hand, triceps of the right and left shoulder, radial flexor of the right hand, large and latissimus dorsi |
Working with pliers and pliers | Flexion of the right hand in the metacarpophalangeal and interphalangeal joints (strength work) | Superficial and deep flexors of the fingers, interosseous and vermiform muscles |
Hacksaw work | Flexion of the fingers of the hand, mainly the right one, extension in the elbow joints and extension movements in the shoulder joints (work to increase the scope and strength) | Finger flexors, triceps brachii, latissimus dorsi |
For the development of movements in the lower extremities, work on a foot sewing machine is used. Work on a foot machine with a restorative purpose is used for injuries of the lower extremities; joint contractures, as well as for the prevention of contractures and faster recovery of movements in intact joints after removal of plaster casts. It is advisable to work on a foot sewing machine with paresis of the foot as a result of damage to the peripheral nerves of the lower extremities to restore function and normalize tone. The main tasks are: 1- increase in range of motion; 2- normalization of muscle tone; 3- uniform increase in the strength of the extensor muscles and flexors of the lower leg. In parallel with this, blood and lymph flow, regeneration processes, tissue metabolism improve, and the strength and tone of the quadriceps femoris muscle increase (conditions are created for its work in isometric mode). The training methodology depends on the task at hand. If it is impossible to work with one sore leg, then it is necessary to start work with the help of a healthy leg, fixing the sore leg so that it does not lag behind the support area. After 5-7 lessons, when the work of the sore leg becomes possible, it is necessary to increase the time of continuous movement of the leg with the parallel development of sewing. To improve the extension or flexion of the foot, supports should be used, starting at 2 cm with a gradual increase in its thickness. To increase the angle of extension of the foot, the stand is placed under the toe, and to increase the angle of flexion - under the heel. The supports should be of different thickness - from 2 to 8 cm. The improvement in strength indicators is determined by the time of work at a given speed until fatigue occurs. The indicator of fatigue will be either turning the flywheel in the opposite direction, or reducing speed, or stopping work. The work time for trauma patients is from 2 minutes at the beginning to 10 minutes or more before discharge. It is desirable to combine thermal procedures (paraffin) with work on a foot machine.
Options for the nature of work in sewing work
Table 3
Type of work | Movements performed | Working muscles | |
Cut (both hands) | Opposition of 1 finger, flexion and extension of fingers (incomplete grip) | Opposite finger 1, interosseous, vermiform, extensor digitorum common | |
Needle work, darning (both hands) | Grabbing the fingers of the left hand, holding the needle with 1, 2 and 3 fingers, pronation and supination of the forearm (incomplete), flexion and extension in the wrist joint | Flexors of fingers 1, 2 and 3, opposing finger I, pronator and supinator, radial and ulnar flexors and extensors of the forearm | |
Sewing on buttons (both hands) | Holding the needle with 1, 2 and 3 fingers of the right hand, bending the 3rd fingers, pronation and supination of the forearm | Opposing finger 1, flexors of fingers 2 and 3, pronators and supinators of the forearm | |
Work on Incomplete finger grip Finger flexors hand sewing right brush, machine movement in the wrist joint, radial and ulnar (both arms) abduction and flexion flexors and extensors, | Incomplete finger grip Finger flexors right hand, circular right hand, movement in the wrist joint, abduction and flexion of the first finger of the left hand | Flexors of the fingers of the right hand, radial and ulnar flexors and extensors abductor 1 finger of the hand, interosseous and vermiform muscles | |
Working on a foot sewing machine | Holding the material with fingers (right and left hand), flexion and extension in the ankle joint | Interosseous and vermiform, extensor digitorum genus, tibialis anterior, triceps tibia | |
With severe damage to the lower extremities, patients adapt to sedentary manual labor. Injuries of the peripheral nerves of the upper extremities. If the median nerve is damaged, occupational therapy is directed to finger flexion (work related to holding and assembling small parts, work with a chisel, chisel, etc.). Restoration of the function of the radial nerve is provided by training in extension of the hand and fingers and abduction of 1 finger (tying threads, folding envelopes, typing, working with a planer). In case of damage to the ulnar nerve, working operations include dilution of the IV and V fingers, extension in the interphalangeal joints (weaving, knitting, cutting, modeling from plasticine, etc.). Some special tasks of occupational therapy and how to solve them: 1. Increased range of motion in the joints of the upper limbs. 2. Increased muscle strength of the upper limbs. 3. Finger grip training (cylindrical, forceps, ball). These tasks are solved, for example, by working with a percussion instrument (hammer, mallet, ax); work with clay or plasticine - modeling; winding threads into balls of different diameters; smoothing sheets of paper, cardboard, fabric; shifting balls and buttons, ironing linen, gluing envelopes. All sewing and shoe manipulations are based on the work of the hand and fingers. 4. Improving the ability of the fingers to produce finely coordinated movements - drawing up a composition from a mosaic; sewing on buttons; embroidery; knitting or crochet. 5. Reducing violations of the sequence of individual movements - imitation of shaving (without a razor); give a spoon and a glass, asking to stir the tea. 1) Decrease in the level of imitation movements - shifting objects from place to place. 2) Learning or improving construction, assembling a whole from separate parts or drawing - building geometric shapes from sticks, assemble a composition from a mosaic. Occupational therapy for depression Often, elderly patients cannot cope on their own with the solution of specific problems (psychological, physical, social, economic) that arise in various stressful situations (changes in the usual way of life, retirement, separation from children, loneliness, deterioration of physical well-being, family conflicts) against the background of which there are neuroses of late age, psychosomatic diseases, depression, anxiety-depressive syndromes and other neurotic symptoms. At present, aging is considered as a phase of life, the course of which is multifactorially determined by the past, present and orientation towards the future, which manifests itself “as a biological, financial, economic, epochal and ecological fate” (I. Ler, 1979). The behavior of an elderly person is determined not so much by the objective moments of the situation as by the form and nature of their subjective perception and experience. As a result, a multilateral orientation of intervention measures (psychological, occupational therapy, social, etc.) is necessary. Memory training. There are 3 main ways to remember: Mechanical ("cramming"); Logical or meaningful (logical or semantic connection); Mnemotechnical (memorization according to certain rules or associatively translated into another sign system, into other images that are easier to remember). A group of patients with a slight decrease in memory is formed. Everyone is invited to introduce themselves, say their name and try to remember the names of other members of the group. The following is a series of exercises. 1. Within 3 minutes, patients are asked to observe the movement of the second hand on the watch. 2. Exercise "fly". Each is given a sheet with a nine-celled 3x3 playing field drawn on it. The essence of the task is that the movement of the “fly” (a pencil placed in the center of the sheet) from one cell to another occurs on command (up, down, right, left) to the neighboring cell. Participants must monitor the movement of the "fly", not allowing it to leave the playing field. Exercise requires constant concentration and trains attention. 3. "Replaying the story" STORY: The ship entered the bay (1), despite the heavy seas (2). Night stood at anchor (3). In the morning we approached the pier (the sailors were released ashore (5 people went to the museum (7.8) 8 sailors decided to just walk around the city (9.10). By evening, they all got together (11), went into the city steam (12) , had a hearty supper (13). At 23 o'clock everyone returned to the ship (14,15). Soon the ship went to another port (16). The patient is asked to remember, write down and read the content of the text. The order of presentation of the fragments is not taken into account. 4. Residents are invited to complete a series of exercises for attention: the essence of the task is to compile a logical chain of selected pictures, followed by a story about this story. Practical communication training (establishing contact) 1. The occupational therapy instructor invites the group members to sit in a large semicircle. He asks each of the participants in turn to go to the center and try by any means available to him, without using speech, to establish contact with each participant in the lesson. After that, the occupational therapy instructor focuses the attention of participants on the means and signs that indicate that contact has been made. 2. The group is divided into two subgroups, which are located in a semicircle (standing or sitting). Participants in the exercise are asked to take turns leaving their semicircle and turning their backs to it. Members of his subgroup will ask him any questions that need to be answered by naming the questioner. The order in the subgroups is optional. During the exercise, group members remember names more easily. 3. Participants sit in a circle. The occupational therapy instructor asks group members to imagine that they are all on a camping trip together. In the center of the circle is an imaginary backpack that you need to pack for the trip. This must be done without words. Everyone carefully monitors what each of the participants puts in their backpack, trying not to repeat themselves. During the exercise, communication skills are improved, contact is established between group members, mood improves. Sensitivity training (the ability to observe, see, hear - perception training) 1. The occupational therapy instructor asks the participants to sit in a circle, he himself goes outside and gives the task for the exercise, standing behind the circle: “You have two minutes during which you need to carefully look at each other.” After the time has elapsed, the occupational therapy instructor asks everyone to turn their backs in their chairs in a circle, approaches one of the group members and says, referring to him, for example: “Ivan Ivanovich, I walk in a circle and pass one, second, third, stop near the fourth person (to the right or left of the participant). Who is this?" If the answer is not correct, then repeat the question and give time to think. After a correct answer, the occupational therapy instructor asks the participant to describe the appearance of the group member next to whom he is standing (clothing, hair color, eye color, etc.). A similar task is given to all members of the group in turn. 2. Group members sit in a circle. The occupational therapy instructor invites the group members to check how well each of them has developed a sense of time. Further, he asks to close your eyes and try after the command “Start!” catch the moment when a minute passes. In this case, you do not need to count for yourself. As soon as the participants think the minute has passed, the occupational therapy instructor asks them to open their eyes and raise their hand, while sitting silently until everyone opens their eyes. During the exercise, the occupational therapy instructor records all participants who: raise their hand before the minute is up; raise their hand in a timely manner; raise their hand later. After completing the exercise, the occupational therapy instructor reports the results of his observations to the participants and invites them to share their impressions. 3. Group members are divided into pairs and sit opposite each other. The occupational therapy instructor gives the task to the group members: each of the participants of the couple in turn says one phrase, starting with the words “I see ...”, the content of which relates to the external appearance of the partner. For example: "I see that your hands are on your knees"; "I see that you have looked to the right"; "I see you bow your head." During the exercise, participants should refrain from using evaluative concepts. This exercise allows you to realize the difference between what “I see” and what “I imagine, interpret”, “it seems to me”. Creativity training (creative thinking) 1. Members of the troupe sit in a circle. The occupational therapy instructor is holding a ball. Patients are encouraged to throw the ball to each other. The one who throws the ball says one of three words: “air”, “earth”, or “water”, and the one who catches it says if the word “air is the name of the bird; “Earth is the name of the animal; “Water is the name of a fish. You need to react as quickly as possible. As the work progresses, the occupational therapy instructor encourages participants to pick up the pace. The exercise is aimed at developing fluency of thinking. 2. Patients are asked to sit in a circle. Occupational therapy instructor holding a ball. The ball is passed to any member of the group. The task is given as follows: “Now you will throw this ball to each other, while whoever throws the ball calls any color, and whoever catches it calls an object of that color. Be careful and try not to repeat those colors and objects that have already been named. Each member of the group is given the opportunity to participate in the exercise. The use of the word "object" rather than the subject gives more opportunities for generating associations. 3. All members of the group sit in a circle. The ball is held by one of the participants in the lesson. He is invited to throw the ball to one of those sitting in a circle and say where the one to whom the ball is addressed will be, while you can send your partners to the most unusual, even fantastic places (in the refrigerator, in ancient Greece, on a palm tree ...). Having caught the ball, you must quickly name three items that you need to take with you, to where the participant in the exercise was sent. It is necessary to be careful not to repeat those places where “others” have already visited, and those objects that have been named. Exercise contributes to the development of imagination, flexibility, originality of thinking. Despite the foregoing, in many patients, with a generally positive attitude towards the measures taken, the attitude towards drugs still prevails, which, apparently, depends on the passive position and the ingrained traditional view of the elderly about treatment. Given that a person constantly interacts with the environment, participates in any events, constantly communicating with people, learning something and receiving information from the outside, it is necessary to include in rehabilitation methods for people with neurosis of late age, depression, occupational therapy, taking into account patients' hobbies. This type of work activity stimulates and shapes the interests and future hobbies of the patient, setting him up for cooperation with an occupational therapy instructor, with the continuation of some activities at home, in a family team. Adaptation through labor is based on a humanistic approach to solving the problems of an elderly person. The attention of psychology is focused on occupational therapy by employment as the basic fundamental need of a healthy person, which has a huge therapeutic effect, since it is a tool for developing normal adaptive capabilities of a person and training the necessary skills (stimulation with wall newspapers, news, reading). Reading is considered as a factor that distracts from thoughts about the disease, helps to endure physical suffering and is considered as an auxiliary part of the healing process for neuroses and psychosomatic diseases. A psychologist with an occupational therapy instructor (if possible with a bibliographer) select literature that has the maximum similarity between the situation in the book and the situation in which the patient is. On the recommendation of a psychologist, an occupational therapy instructor helps (using all areas of work of the occupational therapy room) elderly people with neuroses to maintain and continue to manifest and develop their capabilities, strive to actualize their personal potential, based on Maslow's motivation models: Physiological needs (food, water, sleep) Security needs (stability, security, order) Need for love and belonging (family, friendship) The need for respect (self-respect, recognition) Needs of abilities (development of abilities) In accordance with this, the task of an occupational therapy instructor is to help a person in self-actualization of himself even in old age. Occupational therapy for speech disorders Basic terms: dysarthria- violation of sound pronunciation, tempo, rhythm of speech, discoordination of the process of speaking and breathing. Aphasia- violation of all types of speech activity (oral speech, speech memory, speech understanding, as well as other higher mental functions: reading, writing, orientation in time and space, etc.). An elderly person often has a problem with the purposeful movement of the hand and fingers. Usually this phenomenon is a consequence of cerebral hemorrhage and is often accompanied by a speech disorder. It is known from anatomy that the center of speech is located close to the motor center of the hand. Many authors have proved that the development of the hand is closely related to the development of speech. Thus, in occupational therapy, the main goal should be the development of actions with objects, which positively affects the formation of not only cognitive mental processes, but also the activation of speech function. For the development of manual skill, you can offer: Kneading plasticine, clay with fingers; Roll pebbles, beads, etc. with each finger in turn; Fasten buttons, hooks, zippers, locks on a special training board; Sewing, knitting. In addition, in the form of group therapy, art therapy can be carried out, which helps to create positive emotions in a non-speaking patient (aphasia), which facilitates communication with others through drawing. In the process of these classes, you can use aromatherapy, which will create an atmosphere of comfort and emancipation. It is advisable to include those living with speech impairment in a group with normal speakers, so that by any means they can reach an understanding between them. One of the speech methods is the method of disinhibition of speech, which can be used with all patients of geriatric age. This method includes: Negotiating proverbs, sayings (first the first part of the proverb is said, and then the task is complicated by the fact that only the second part is said). If the patient cannot say, then on special cards he selects the right answer. Singing well-known songs (you can use a tape recording). In most patients who have passed the age of sixty, speech memory suffers. For memory training and a detailed statement, it is good to use short texts that correspond to the interests of patients, which it is desirable to retell, and, if necessary, leading questions are selected to the context. CONCLUSION Occupational therapy, by right, deserves wider use in the rehabilitation of the elderly. First of all, it is occupational therapy by employment, household rehabilitation, restorative occupational therapy, training methods. The effectiveness of occupational therapy has been proven by practice. The beauty of this method lies in: 1. Ease of use of occupational therapy with low material costs for its organization; 2. Availability of use at all stages of rehabilitation, including at home; 3. Variety, which is provided by a large number of exercises as a result of a combination of different labor movements and operations; 4. Good compatibility with almost any area of treatment, including in complex rehabilitation programs (with physiotherapy, exercise therapy, psychotherapy, etc.). Besides: Participation in any labor operation, restoration of self-service skills increases the patient's self-esteem, eliminates his idea of his own inferiority, provides a good emotional background and a better mutual understanding between staff and patients; Collective work restores impaired communication skills. The technique does not carry an additional drug load, and in some cases, when using occupational therapy, it is possible to reduce the dose of medications taken. | |||
Used Books:
Information and methodological publication "Older people: social policy and development of social services" under the general editorship of Moscow 2003.
Collection of information materials "Introduction of new forms of social services for the elderly and disabled" interregional seminar St. Petersburg 2005.
For records
_______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
government agency
Center for Social
services for the population of the city of Volsk "
Director of the CSC in Volsk
Valery Aleksandrovich Katkov
Our address:
412900 Volsk, Saratov region
E-mail address:
*****@***ru
Phones:
Administrative building
(Secretary): 8(845-
The information material was compiled by a specialist in the organizational and methodological department
Edition of 10 copies.